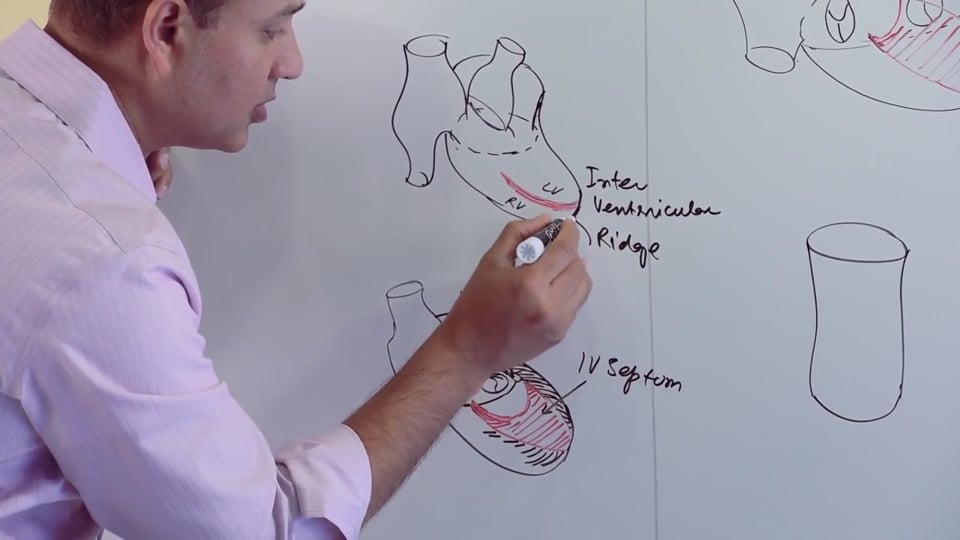
Embryology and fate of the pharyngeal arch artries.
STUDY NOTES:
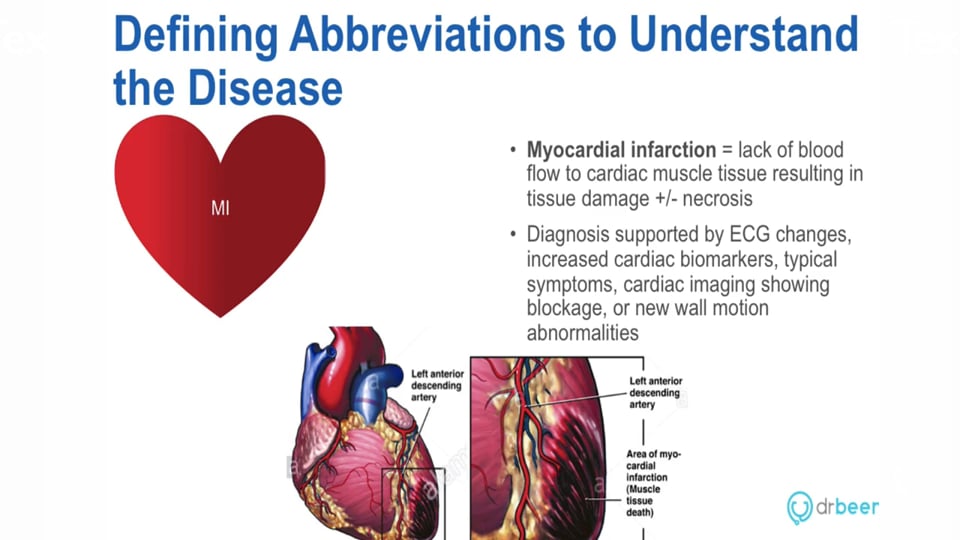
PHARYNGEAL ARCH ARTERIES
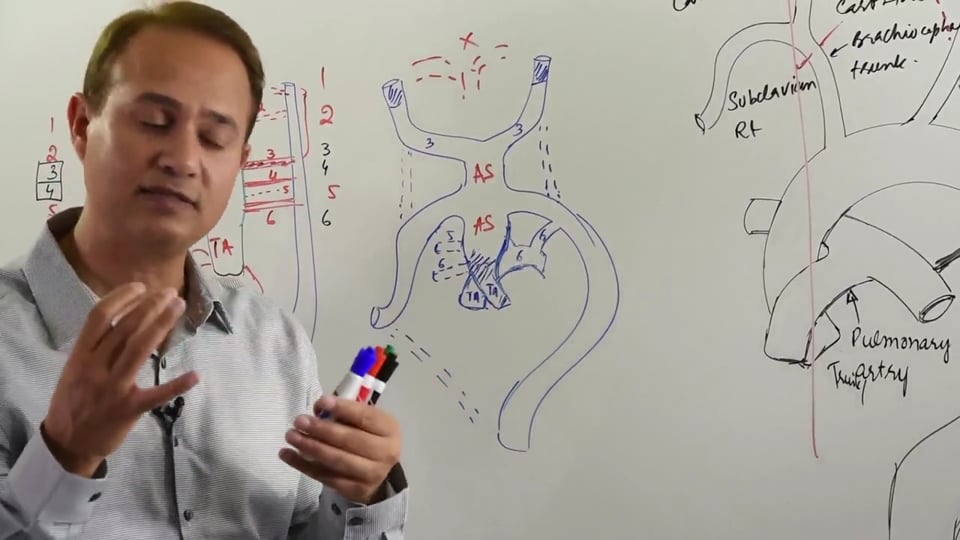
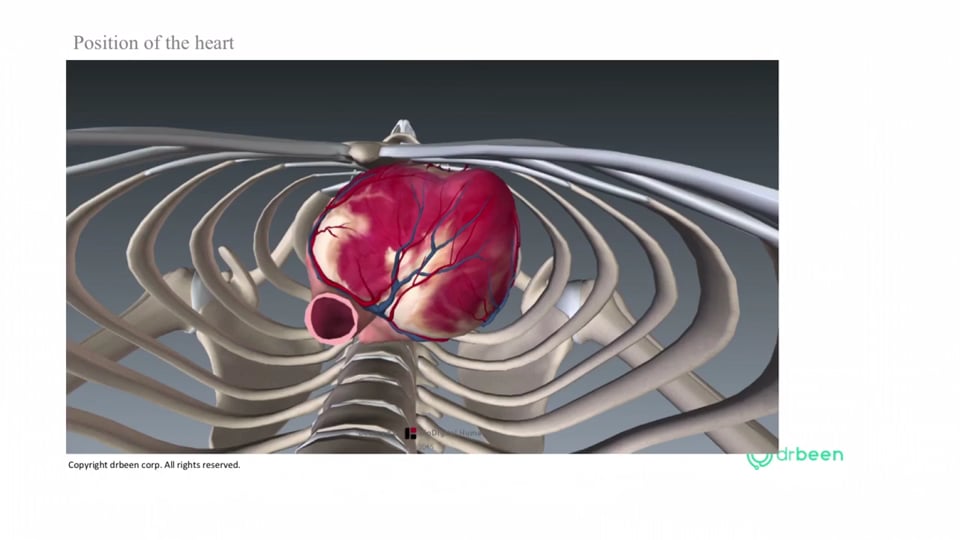
The aorta arises from the left ventricle as its outflow tract. Aorta forms an arch before descending downwards as the thoracic/descending aorta. This arch of aorta gives rise to three arteries; from right to left these arteries are the, left common carotid and the left subclavian artery. On the right side the brachiocephalic trunk gives rise to right subclavian artery and then continues as the right common carotid artery which eventually divides into internal and external carotid arteries of the right side. The left common carotid artery is a direct branch of arch of aorta and it ends up dividing into external carotid and internal carotid arteries of the left side. Finally the left subclavian artery arises from the arch of aorta prior to the ductus arteriosus, after which the arch curves downwards and continues as descending or thoracic aorta.
As the embryo is developing, two dorsal aortae develop on either side and give off branches to oxygenate ventral and dorsal parts of the embryo. Simultaneously the pharyngeal arches develop along with their pharyngeal arteries. There are six pharyngeal arteries that develop. The first two pairs of pharyngeal arteries develops by the 3rd and 4th week and the sixth pair develops by the 6th or 7th week. By the time the last pair (6th pair) of the pharyngeal arteries develops, the first and second pair of pharyngeal arteries has degenerated. It's important to remember that all six pairs of pharyngeal arch arteries aren't present at the same time. The 1st and 2nd pharyngeal arch arteries give rise to part of Maxillary artery and Stapedial artery respectively. Other than that the first two pharyngeal arch arteries degenerate. The 3rd pharyngeal arch artery is of importance, as it combines with the adjacent part of dorsal aorta to form common carotid and proximal part of the internal carotid arteries. The 4th pharyngeal arch artery on the right side gives rise to Brachiocephalic trunk part before the origin of common carotid artery while the left side it gives rise to the aortic arch. The 5th pharyngeal arch artery normally doesn’t develop in humans. However, in cases where it does develop, it tends to be rudimentary and degenerates soon.5th pharyngeal arch artery regresses and degenerates. The 6th pharyngeal arch artery gives rise to ductus arteriosus on the left side and it regresses on the right side.
On the right side, the 1st, 2nd, 5th and 6th pharyngeal arch arteries tend to regress (completely or partially) whereas, the 3rd and 4th are of importance in terms of giving rise to adult structures. On the left side 1st, 2nd and 5th pharyngeal arch arteries tend to regress (completely or partially), whereas the 3rd, 4th and 6th give rise to arterial structures. This above information is summarized in the table overleaf:
|
Aortic arch derivative
|
Arterial structure formed on the right side |
Arterial structure formed on the left side |
|
1st (Maxillary artery)* |
degenerates |
degenerates |
|
2nd (Stapedial artery)* |
degenerates |
degenerates |
|
3rd pharyngeal arch artery |
Common carotid & proximal part of the internal carotid arteries |
degenerates |
|
4th pharyngeal arch artery |
Proximal part of the Brachiocephalic artery |
Aortic arch, rest of it degenerates |
|
5th pharyngeal arch artery |
degenerates |
Degenerates |
|
6th pharyngeal arch artery |
proximal parts of pulmonary arteries of both sides, rest of it degenerates |
Ductus arteriosus |
So what happens is, that the first two pharyngeal arch arteries degenerate and the third one ,as mentioned earlier, is directly connected to the dorsal aortae on either side. The parts of dorsal aortae connected to the 4th, 5th and 6th pharyngeal arches tend to degenerate as well. As a result the 3rd pharyngeal arch arteries on either side get directly connectedin the middle to the aortic sac. Inferiorly, the aortic sac is connected to the truncus arteriosus which at this point is undergoing septation to form aorta and the pulmonary trunk. So, the initial part of the pulmonary trunk is formed by the truncus arteriosus whereas the point where the pulmonary trunk bifurcates into two pulmonary arteries (proximal parts of pulmonary arteries) is formed by the 6th pharyngeal arch artery.
Eventually, the 3rd pharyngeal arch (which is directly connected to the aortic sac) starts dividing along with the aortic sac. This division eventually results in the brachiocephalic trunk developing on the right side. On the left side, part of the 3rd pharyngeal arch forms the aortic arch. Common carotid and part of internal carotid arteries on both sides are formed by the 3rd pharyngeal arch artery as well. However, distal part of internal carotid is formed by the dorsal aorta.
The fate of dorsal aorta is different on either side. On the right side, the dorsal aorta ends up forming the right subclavian artery. On the left side however, the dorsal aorta forms a part of the descending aorta and the arch of aorta. Aorta primarily forms from the aortic sac. Although, part of aorta that is proximal to the commencement of the common carotid artery on the left side, is formed by the artery of the 4th pharyngeal arch. On the right side as well, the part just before the commencement of the common carotid artery from the brachiocephalic trunk is formed by the 4th pharyngeal arch artery. Right Subclavian artery forms from the dorsal aorta, whereas the left subclavian artery forms from existing vasculature as part of angiogenesis.
On the right side, the right vagus nerve gives rise to right recurrent laryngeal nerve which passes under the right subclavian artery to ascend towards the larynx region. On the left side, the left vagus nerve gives rise to left recurrent laryngeal nerve which hooks around the ligamentum arteriosum and further curves under the aortic arch to ascend and reach the larynx. On the right side, part of the 6th pharyngeal artery tends to degenerate hence the right recurrent laryngeal nerve has to pass behind the right subclavian artery on, as it courses upward.
An important clinical correlate to remember is that, as the left recurrent laryngeal nerve curves under the arch of aorta, it can get damaged by aortic arch aneurysm or a malignancy. Left recurrent laryngeal nerve damage can result in paralysis of the left vocal cords. On the right side, since right recurrent laryngeal is unaffected by any aortic arch pathologies because it arises from the right vagus nerve in the root of the neck and subsequently passes under the subclavian artery (and not under the arch of aorta).
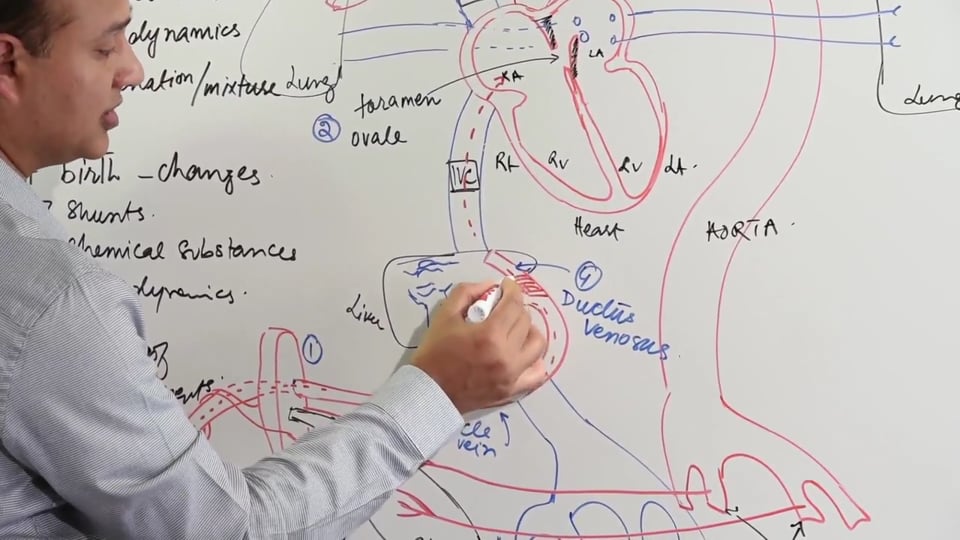
Ligamentum arteriosum is the embryologic remnant of the ductus arteriosus. Ductus arteriosus itself arises from the left 6th pharyngeal arch artery. Ductus arteriosus opens into underside of the arch of aorta (distal to origin of the left subclavian artery) and it functions to form a shunt which allows the flow of deoxygenated blood from the pulmonary trunk to the aorta (right to left shunt). This right to left shunting allows the deoxygenated blood to complete bypass the pulmonary circuit.
COARCTATION OF AORTA
Coarctation of aorta is a constriction of the aorta just after it has given rise to subclavian artery. Post the coarctation site, the aorta becomes significantly narrowed and the blood supply to the lower limb and the abdomen is diminished which results in weak pulses of the lower limb. As compensation, over time collaterals develop around the chest wall and the abdomen to supply the lower body. Coarctation of aorta also affects the heart, which now has to pump against greater peripheral resistance and hence at a higher pressure in order to maintain peripheral circulation, thus it may lead to cardiac failure in severe cases.
It's important to understand the underlying cause for this coarctation of aorta. During development, the ductus arteriosus is composed of a specialized smooth muscular contractile tissue. This specialized contractile tissue at times makes its way into the arch of aorta. Hence, after birth when this migrated contractile tissue contracts and tends to narrow the aortic lumen (similar to obliteration of ductus arteriosus in response to increased oxygen and decreased PGE levels), there's a resultant coarctation of the aorta. Alternatively,developmental alteration can also result in the coarctation of aorta.
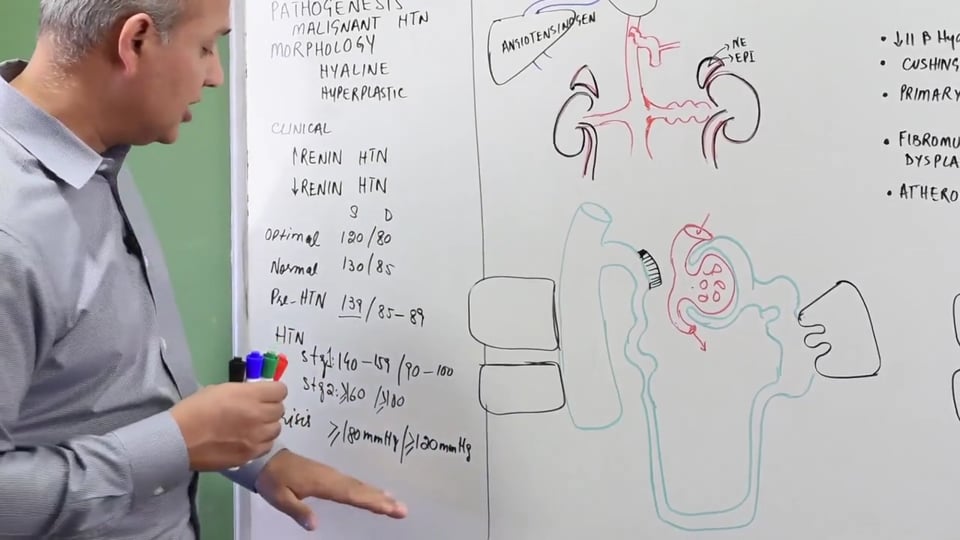
Clinically, coarctation of aorta manifests with the following:
Coarctation of aorta is divided into two types based on the location of the narrowing of aorta with respect to the position of ductus arteriosus:
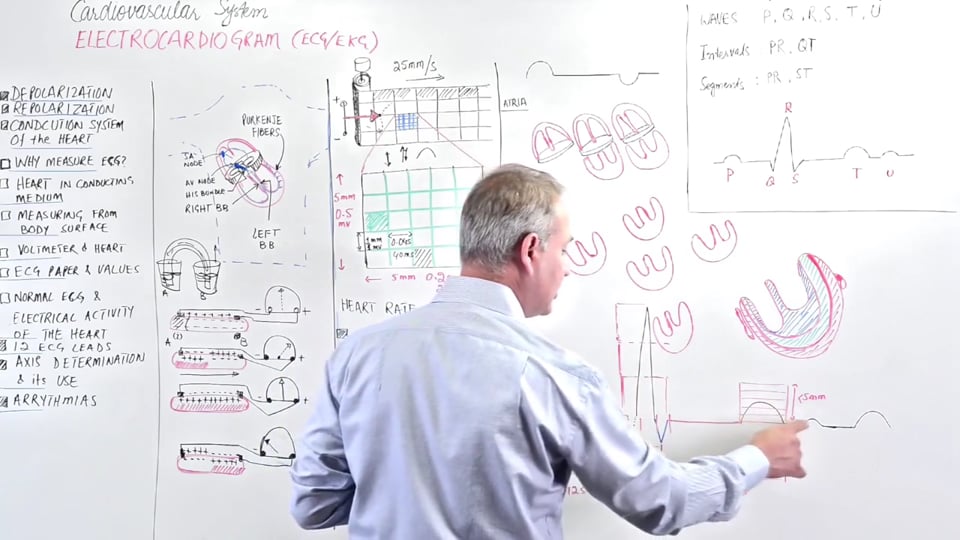
In this video we will learn about pharyngeal arch arteries:
1. Aortic arteries.
2. Truncus arteriosus.
3. Dorsal aorta.
4. 3rd pharyngeal pouch.
5. 4th pharyngeal pouch.
6. 6th pharyngeal pouch.

MD., MSc., MSc., BSc
Mobeen Syed is the CEO of DrBeen Corp, a modern online medical education marketplace. Mobeen is a medical doctor and a software engineer. He graduated from the prestigious King Edward Medical University Lahore. He has been teaching medicine since 1994. Mobeen is also a software engineer and engineering leader. In this role, Mobeen has run teams consisting of hundreds of engineers and millions of dollars of budgets. Mobeen loves music, teaching, and doing business. He lives in Cupertino CA.












Write A New Comment
0 Comments