This video is part of the blood flow regulation series. We present the blood flow in a muscle during the resting and active state. Extrinisc vs. intrisic blood flow and the triggering factors are disucssed.
STUDY NOTES:
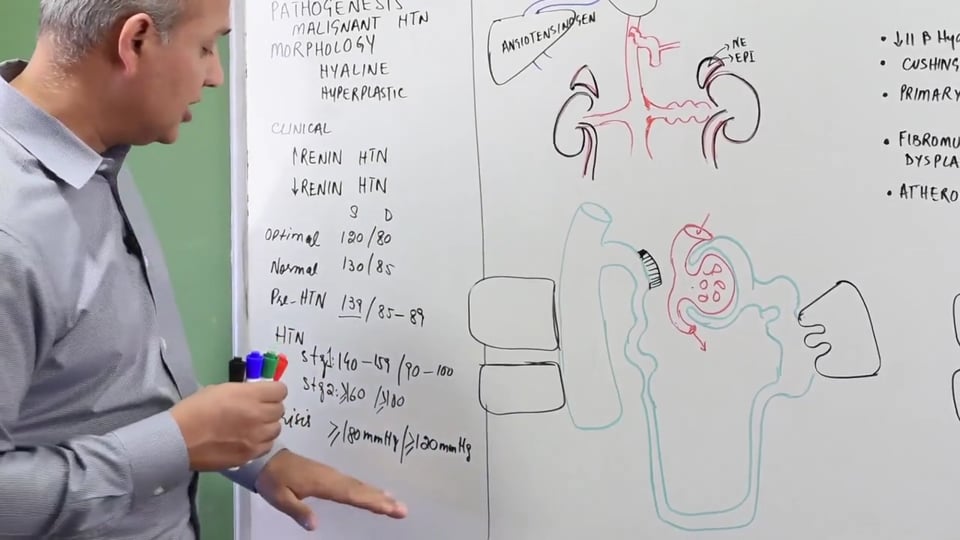
AUTOREGULATION – MUSCLE BLOOD FLOW
The metabolic requirements of a muscle change duringexercise compared to when it is at rest. The blood flow also changes accordingly with the metabolic demands of the muscle. Therefore, the purpose of this lecture is to establish a better understanding of the regulation of blood flow to a muscle, both during rest and exercise. Both of these regulations will be discussed separately:
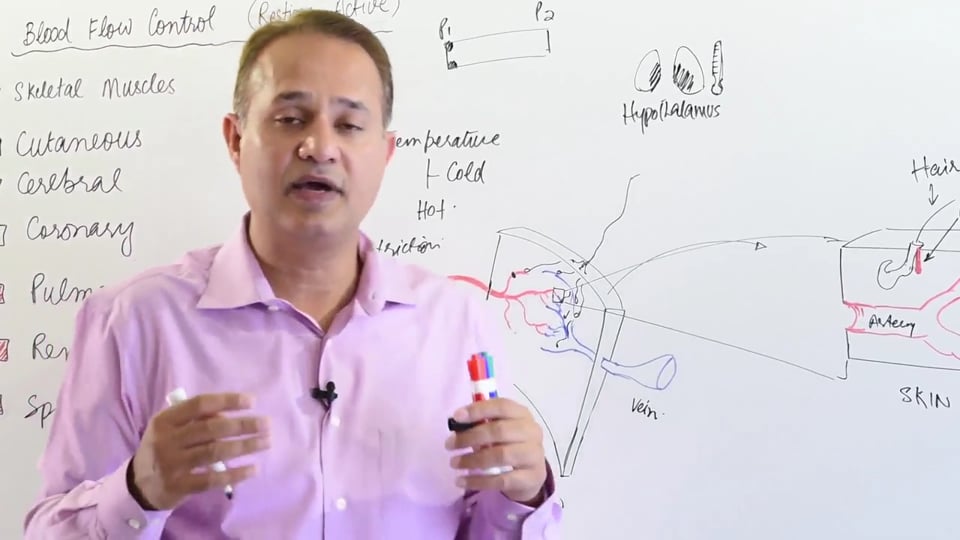
BLOOD FLOW TO A RESTING MUSCLE
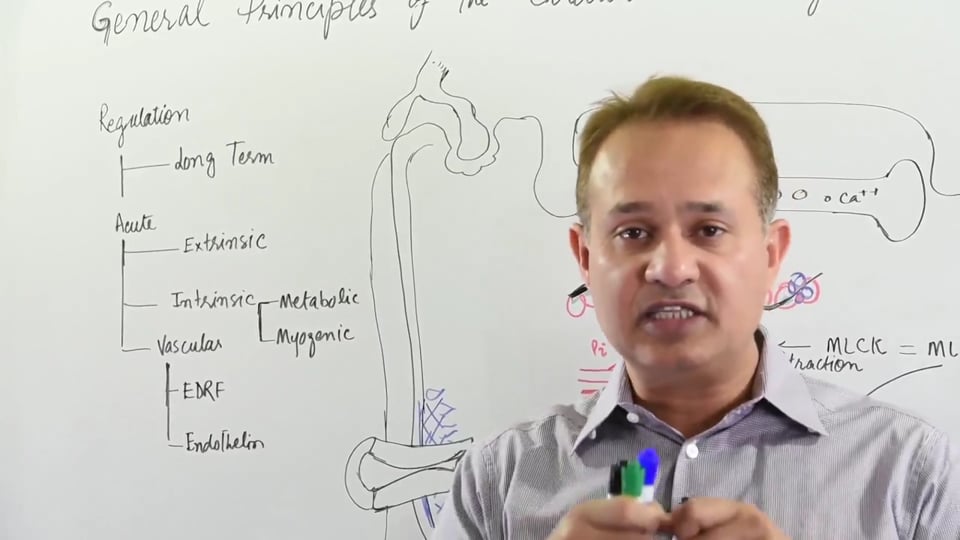
The blood flow to a muscle at rest is controlled globally along with the rest of the body through extrinsic regulation. Blood flow is extrinsically regulated through the following auto-regulatory mechanisms:
• Sympathetic Nervous System [SANS]
• Para sympathetic Nervous System [PANS]
• Hormonal Control
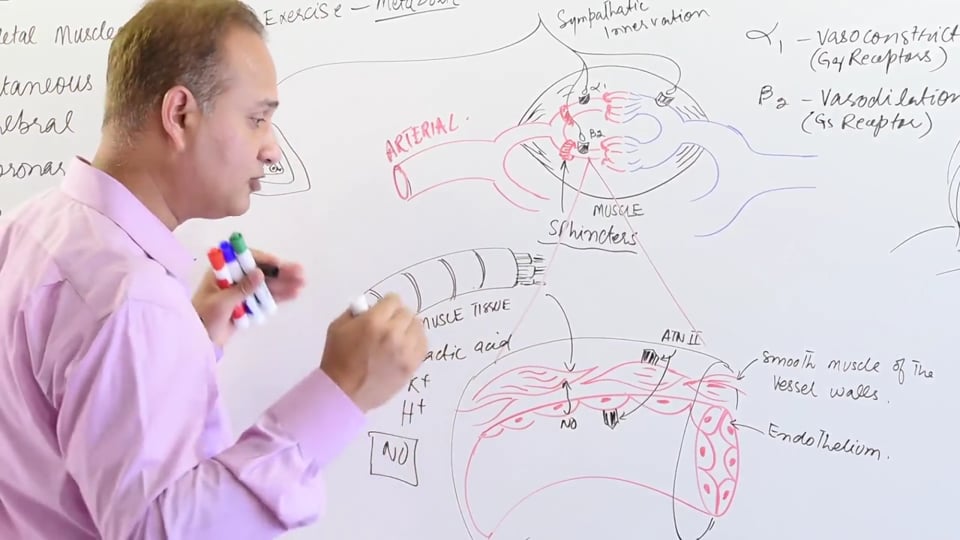
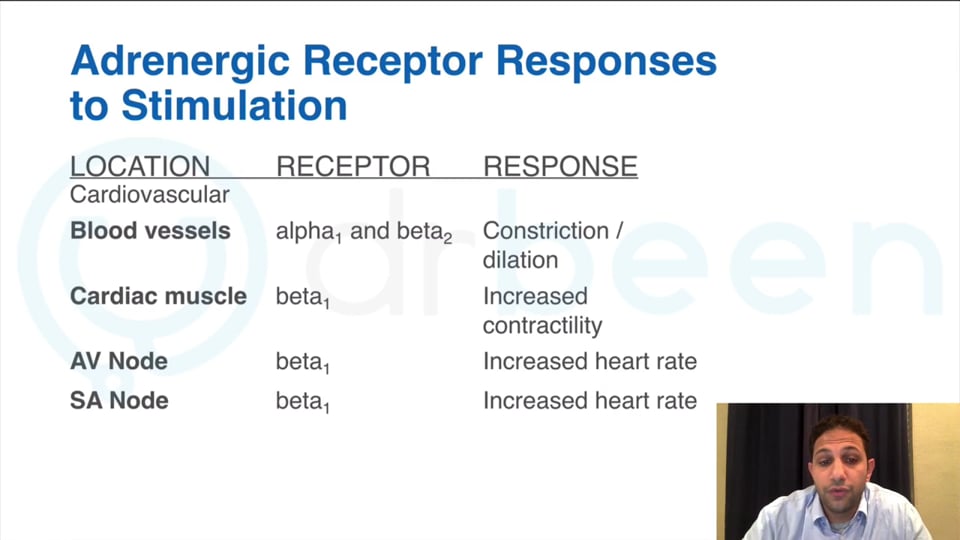
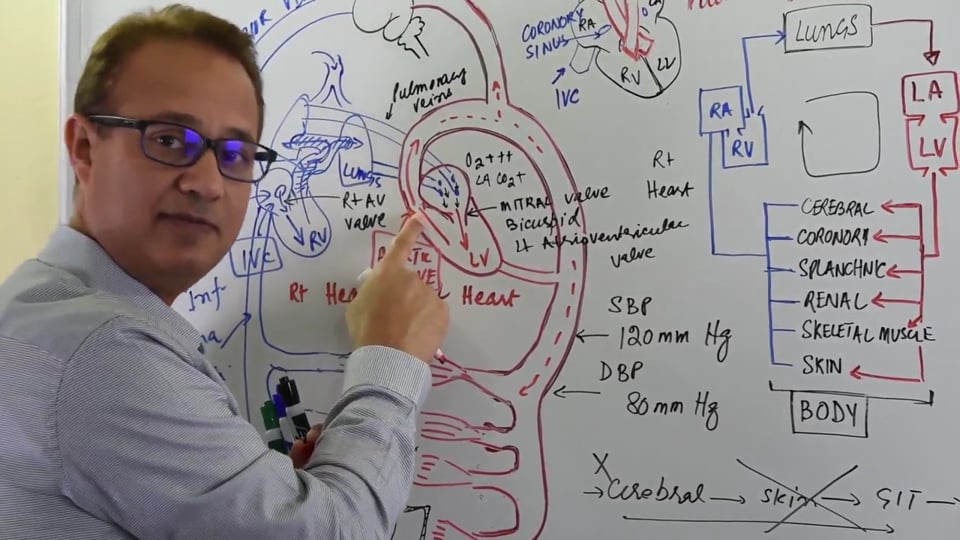
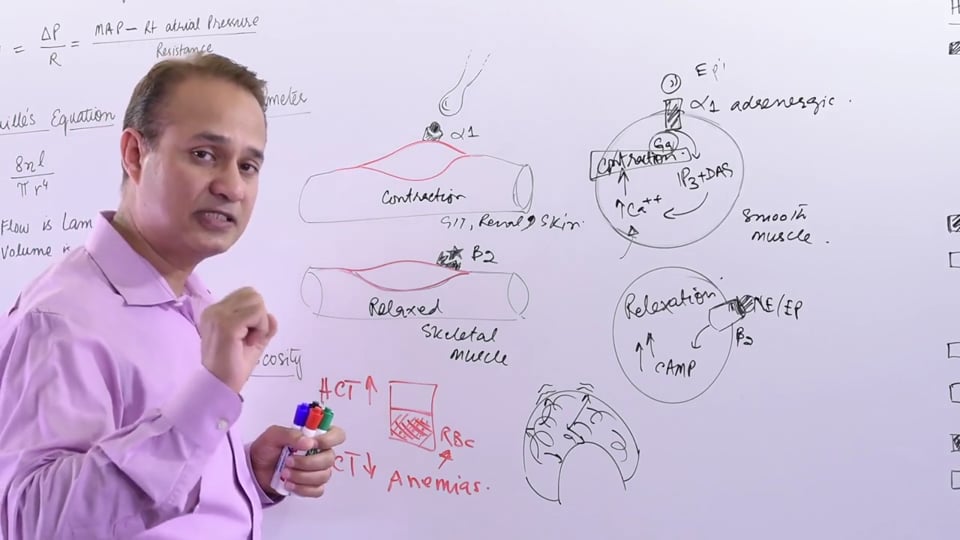
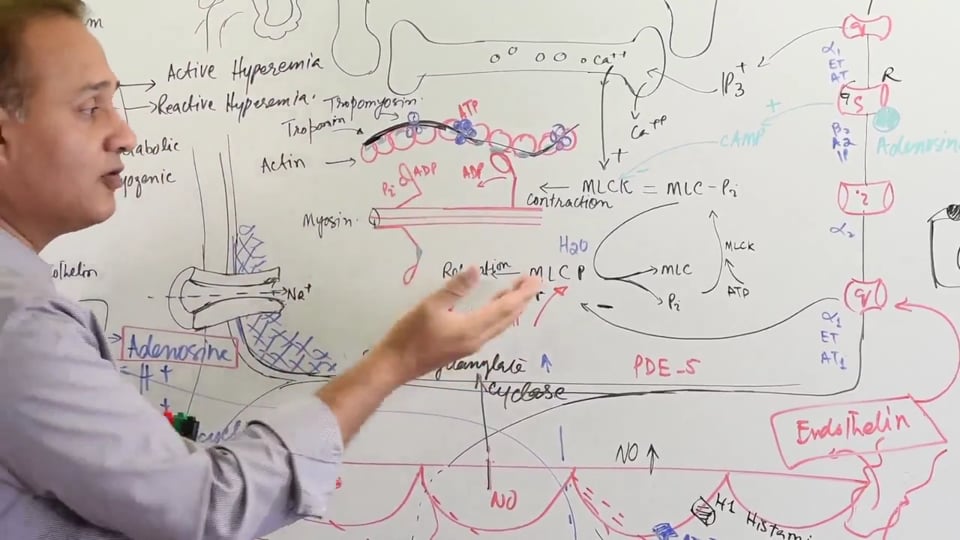
The vascular smooth muscles possess both, alpha-1 (α-1) and beta-2 (β-2) receptors on their surface membrane that are innervated by the SANS. It is worth noting that during sympathetic outflow, the β-2 response is dominant over the α-1 response. This explains why sympathetic stimulation, which occurs in situations of flight and fight, causes the vessels supplying the skeletal muscles to dilate while causing the vessels supplying the visceras i.e. splanchnic, renal and skin to constrict. This allows shunting of maximum amounts of blood towards the skeletal muscles.
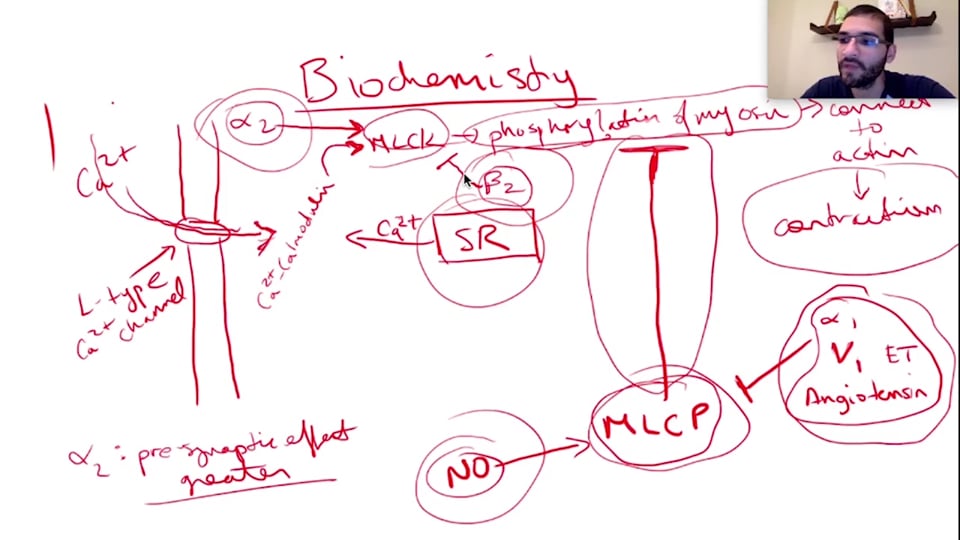
The α-1 receptors are G-q coupled receptors that cause contraction of the vascular smooth muscle upon stimulation. The β-2 receptors are innervated by sympathetic supply as well, but their effect is inhibitory. This is because the β-2 receptors are G stimulatory transmembrane proteins that decrease the intracellular levels of cAMP, thereby causing relaxation of the vascular smooth muscle and vasodilation follows. As mentioned above, the β-2 response is predominant over the α-1 response. However, the response can be shifted towards α-1 if sympathetic overflow occurs. With SANS response, there’s an overflow of epinephrine. At low concentration, epinephrine occupies β-2 receptors and encourages vasodilation of vessels perfusing the skeletal muscle. However, at high concentration, epinephrine occupies α-1 receptors and encourages vasoconstriction of vessels perfusing the skeletal muscle.
So, at rest the blood flow to skeletal muscles is predominantly regulated by SANS. This SANS control is predominantly mediated via the β-2 receptors. Since these receptors are Gstimulatory, the response generated encourages vasodilation.
[Note: In the lecture it’s mentioned that β-2 receptor is G-s coupled. However this is not the case. In fact, β-2 receptors are G-i coupled, and there response is inhibitory. Please correct this.]
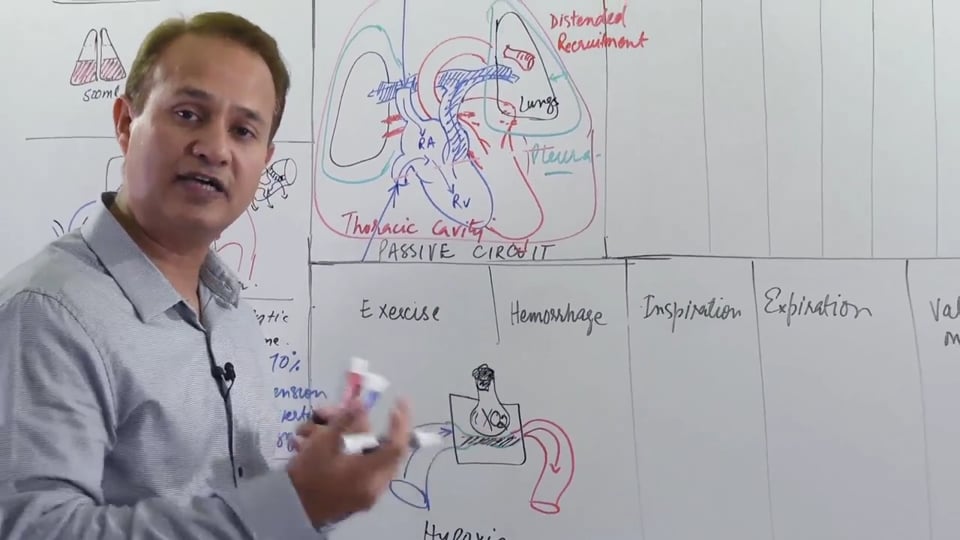
BLOOD FLOW TO AN EXERCISING MUSCLE(ACTIVE STATE)
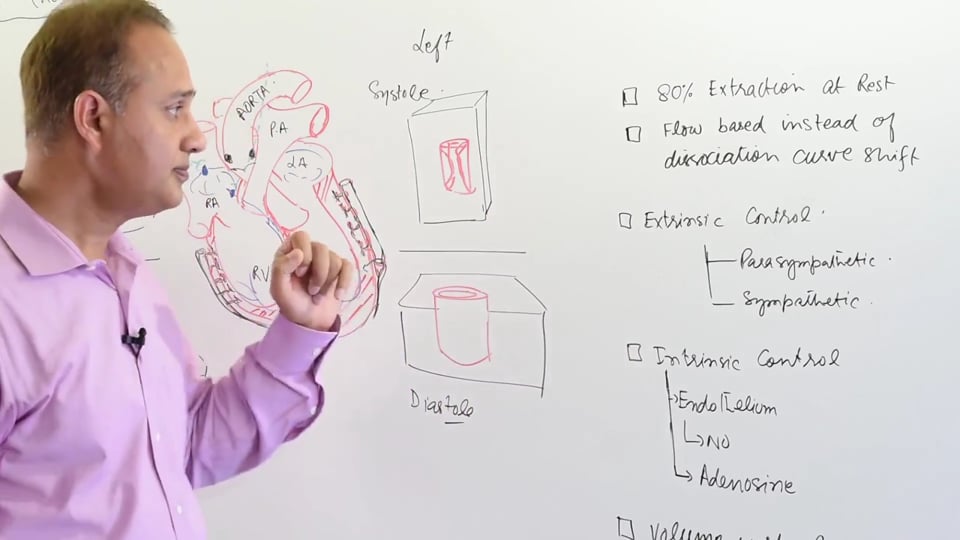
During exercise, the control of vascular smooth muscles becomes totally dependent on intrinsic regulatory factors. The extrinsic control becomes unresponsive and is overwhelmed by the intrinsic control. This is justified by the fact that during exercise, the demand for oxygen and the need to remove metabolic waste increases multiple folds. Therefore, the vascular caliber increases in order to increase blood flow and provide for the increase demand. The factors responsible for intrinsic control are actually waste metabolites that also have vasodilatory properties.
These vasodilator metabolites include the following:
• H+ ions
• Lactic acid
• Carbon dioxide
• Adenosine
• Potassium ions.
These above mentioned metabolites also diminish norepinephrine's ability to vasoconstrict the arterioles. Moreover, the increased endothelial shear-stress of increased blood flow liberates nitric oxide from the endothelium itself. This NO diffuses into the vascular smooth muscle and activates the cGMP pathway via the myosin light chain phosphatase enzyme activation as discussed previously (CVS Physiology Lecture#11: Nitric Oxide). This eventually causesvasodilation.
The skeletal muscles are also responsive to Angiotensin II. Angiotensin II predominantly causes vasoconstriction but it can also cause vasodilation to some extent. The vasodilatingeffect is carried out to balance out the more potent vasoconstricting effect of Angiotensin II. The vasodilating effect of Angiotensin II involves its binding to the ATII receptors on the endothelium which subsequently releases NO. This NO then diffuses into the vascular smooth muscle and causes vasodilation to occur. The Angiotensin II induced vasoconstriction is due to its binding to receptors on vascular smooth muscles.
Also, during exercise the muscle activity increases. This enables the muscles to act as muscular pumps that increase the blood flow and allows for rapid removal of metabolic waste.
SUMMARY
At rest, the blood flow is controlled mainly by the beta 2 activity which leads to vasodilatation
During exercise, the blood flow is taken in control by intrinsic factors that are metabolites with vasodilating properties. The rapidly contracting and relaxing muscles during exercise act as pumps that help increase blood flow.
Finally the endothelium in the local working tissues will create metabolites which will cause vasodilatation.
In this video we will learn about :
1. Blood flow control of skeletal muscles
a. At rest.
b. At contraction.
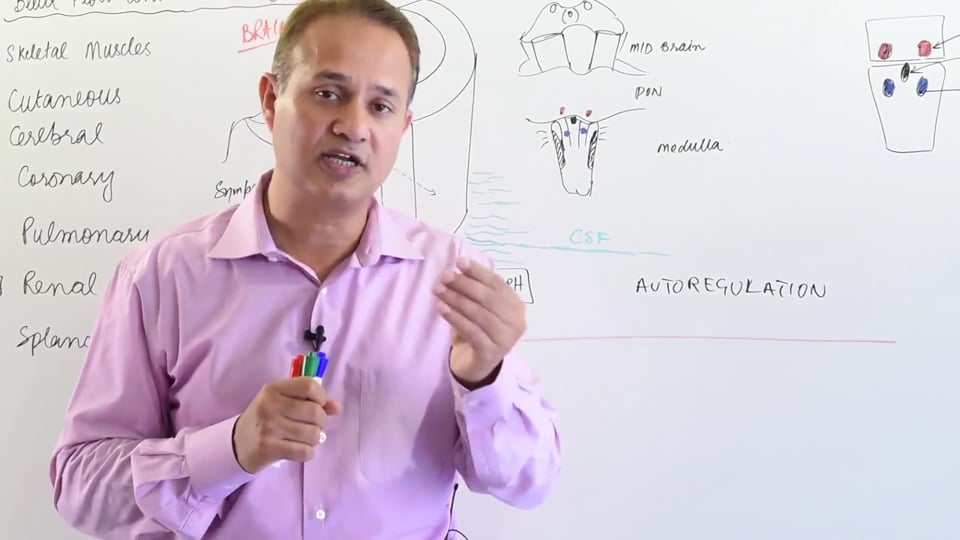
2. Sympathetic innervation of skeletal muscles.
3. Auto regulation of blood flow.
Following answers are created by ChatGPT. Occasionally the answer may be harmful, incorrect, false, misleading, incomplete, or limited in knowledge of world. Please contact your doctor for all healthcare decisions. Also, double check the answer provided by the AI below.
In addition to the presenter, following authors may have helped with the content writing, review, or approval:
ACCME Accreditation Statement
The DrBeen Corp is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to
provide continuing medical education for physicians.
AMA Credit Designation Statement
The DrBeen Corp designates this enduring material for a maximum of 0.25 AMA PRA Category 1
Credits™.
Physicians should claim only the credit commensurate with the extent of their participation in the
activity.
In accordance with the disclosure policies of DrBeen Corp and the ACCME (Accreditation Council for
Continuing Medical Education), we are committed to upholding principles of balance, independence,
objectivity, and scientific rigor in all of our Continuing Medical Education (CME) and Continuing
Education (CE) activities. These policies include the careful management and mitigation of any relevant
financial relationships with organizations that are not eligible.
All members of the Activity Planning Committee and presenters have disclosed their relevant financial
relationships. The DrBeen Corp CE Committee has thoroughly reviewed these disclosures and determined
that these relationships are not deemed inappropriate in the context of their respective presentations.
Additionally, they are found to be consistent with the educational objectives and the integrity of the
activity.
| Faculty | Disclosures |
|---|---|
| Dr. Mobeen Syed | Author declares no conflict of interest. |

MD., MSc., MSc., BSc
Mobeen Syed is the CEO of DrBeen Corp, a modern online medical education marketplace. Mobeen is a medical doctor and a software engineer. He graduated from the prestigious King Edward Medical University Lahore. He has been teaching medicine since 1994. Mobeen is also a software engineer and engineering leader. In this role, Mobeen has run teams consisting of hundreds of engineers and millions of dollars of budgets. Mobeen loves music, teaching, and doing business. He lives in Cupertino CA.

Luis A Verduzco M.D.
Luis A Verduzco M.D.
Ahmed Zaafran, MD
 1.25 CME
1.25 CME
Luis A Verduzco M.D.
Ahmed Zaafran, MD
 0.50 CME
0.50 CME
Tatyana Travkina, MD
Ahmed Zaafran, MD
Ahmed Zaafran, MD
Ahmed Zaafran, MD
 0.75 CME
0.75 CME
Tatyana Travkina, MD
Ahmed Zaafran, MD
Tatyana Travkina, MD
Ana Crawford M.D., M.Sc.
Ahmed Zaafran, MD
Ahmed Zaafran, MD
Ahmed Zaafran, MD
 1.25 CME
1.25 CME
Dr. Mobeen Syed
Ahmed Zaafran, MD
 0.12 CME
0.12 CME
Dr. Mobeen Syed

Ahmed Zaafran, MD
 1.25 CME
1.25 CME
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
 0.50 CME
0.50 CME
Dr. Mobeen Syed
 0.75 CME
0.75 CME
Dr. Mobeen Syed
Ahmed Zaafran, MD
 0.25 CME
0.25 CME
Dr. Mobeen Syed
 0.16 CME
0.16 CME
Dr. Mobeen Syed
 0.50 CME
0.50 CME
Dr. Mobeen Syed
 0.16 CME
0.16 CME
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
 0.75 CME
0.75 CME
Dr. Mobeen Syed
 0.50 CME
0.50 CME
Dr. Mobeen Syed
 0.20 CME
0.20 CME
Dr. Mobeen Syed
 0.20 CME
0.20 CME
Dr. Mobeen Syed
 0.12 CME
0.12 CME
Dr. Mobeen Syed
 0.09 CME
0.09 CME
Dr. Mobeen Syed
 0.24 CME
0.24 CME
Dr. Mobeen Syed
 0.25 CME
0.25 CME
Dr. Mobeen Syed
 0.19 CME
0.19 CME
Dr. Mobeen Syed
 0.08 CME
0.08 CME
Dr. Mobeen Syed
 0.11 CME
0.11 CME
Dr. Mobeen Syed
 0.09 CME
0.09 CME
Dr. Mobeen Syed
 0.50 CME
0.50 CME
Dr. Mobeen Syed
 1.00 CME
1.00 CME
Dr. Mobeen Syed
 0.25 CME
0.25 CME
Dr. Mobeen Syed
 0.50 CME
0.50 CME
Dr. Mobeen Syed
 0.50 CME
0.50 CME
Dr. Mobeen Syed
 0.50 CME
0.50 CME
Dr. Mobeen Syed
 0.16 CME
0.16 CME
Dr. Faraaz Bhatti
 0.50 CME
0.50 CME
Dr. Mobeen Syed
 0.50 CME
0.50 CME
Dr. Mobeen Syed
 0.50 CME
0.50 CME
Dr. Mobeen Syed
 0.50 CME
0.50 CME
Dr. Mobeen Syed
 0.18 CME
0.18 CME
Dr. Mobeen Syed
 0.17 CME
0.17 CME
Dr. Mobeen Syed
 0.50 CME
0.50 CME
Dr. Mobeen Syed
 0.21 CME
0.21 CME
Dr. Mobeen Syed
 0.21 CME
0.21 CME
Dr. Mobeen Syed
 0.50 CME
0.50 CME
Dr. Mobeen Syed
 0.25 CME
0.25 CME
Dr. Mobeen Syed
 0.24 CME
0.24 CME
Dr. Mobeen Syed
 0.50 CME
0.50 CME
Dr. Mobeen Syed
 0.75 CME
0.75 CME
Dr. Mobeen Syed
 0.50 CME
0.50 CME
Dr. Mobeen Syed
 1.00 CME
1.00 CME
Dr. Mobeen Syed
 0.75 CME
0.75 CME
Dr. Mobeen Syed
 0.25 CME
0.25 CME
Dr. Mobeen Syed
 0.08 CME
0.08 CME
Dr. Mobeen Syed
 0.05 CME
0.05 CME
Dr. Mobeen Syed
 0.12 CME
0.12 CME
Dr. Mobeen Syed
 1.25 CME
1.25 CME
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
 0.50 CME
0.50 CME
Dr. Mobeen Syed
 0.22 CME
0.22 CME
Dr. Mobeen Syed
 0.50 CME
0.50 CME
Dr. Mobeen Syed
 0.25 CME
0.25 CME
Dr. Mobeen Syed
 0.13 CME
0.13 CME
Dr. Mobeen Syed
 0.16 CME
0.16 CME
Dr. Mobeen Syed
 0.16 CME
0.16 CME
Dr. Mobeen Syed
 0.15 CME
0.15 CME
Dr. Mobeen Syed
 0.15 CME
0.15 CME
Dr. Mobeen Syed
 0.19 CME
0.19 CME
Dr. Mobeen Syed
 0.75 CME
0.75 CME
Dr. Mobeen Syed
 0.12 CME
0.12 CME
Dr. Mobeen Syed
0.16 CME
Dr. Mobeen Syed
 0.25 CME
0.25 CME
Dr. Mobeen Syed
 0.24 CME
0.24 CME
Dr. Mobeen Syed
 0.25 CME
0.25 CME
Dr. Mobeen Syed
 0.19 CME
0.19 CME
Dr. Mobeen Syed
 0.18 CME
0.18 CME
Dr. Mobeen Syed
 0.50 CME
0.50 CME
Dr. Mobeen Syed
 0.75 CME
0.75 CME
Dr. Mobeen Syed
 0.50 CME
0.50 CME
Dr. Mobeen Syed
 0.25 CME
0.25 CME
Dr. Mobeen Syed
 0.50 CME
0.50 CME
Dr. Mobeen Syed
 0.50 CME
0.50 CME
Dr. Mobeen Syed
 0.25 CME
0.25 CME
Dr. Mobeen Syed
 0.75 CME
0.75 CME
Dr. Mobeen Syed
 0.13 CME
0.13 CME
Dr. Mobeen Syed
 0.50 CME
0.50 CME
Dr. Mobeen Syed
 0.25 CME
0.25 CME
Dr. Mobeen Syed
 0.50 CME
0.50 CME
Dr. Mobeen Syed
 0.50 CME
0.50 CME
Dr. Mobeen Syed
 0.50 CME
0.50 CME
Dr. Mobeen Syed
 0.25 CME
0.25 CME
Dr. Mobeen Syed
 1.00 CME
1.00 CME
Dr. Mobeen Syed
 0.25 CME
0.25 CME
Dr. Mobeen Syed
 0.20 CME
0.20 CME
Dr. Mobeen Syed
 0.25 CME
0.25 CME
Dr. Mobeen Syed
 0.17 CME
0.17 CME
Dr. Mobeen Syed
 0.25 CME
0.25 CME
Dr. Mobeen Syed
 0.50 CME
0.50 CME
Dr. Mobeen Syed
 0.25 CME
0.25 CME
Dr. Mobeen Syed
 0.19 CME
0.19 CME
Dr. Mobeen Syed
 0.50 CME
0.50 CME
Dr. Mobeen Syed
All information contained in and produced by DrBeen corp is provided for educational purposes only. This information should not be used for the diagnosis or treatment of any health problem or disease.
THIS INFORMATION IS NOT INTENDED TO REPLACE CLINICAL JUDGMENT OR GUIDE INDIVIDUAL PATIENT CARE IN ANY MANNER.
Click here for notice and disclaimer.

Write A New Comment
0 Comments