This video presents
- Development of the interventricular septum
- Development of the aorticopulmonary septum
- Clinical points related to these topics
- Patent truncus arteriosus
- Transformation of the great artries
- Tetralogy of fallot.
STUDY NOTES:
VENTRICLES & AORTICOPULMONARY SEPTUM
DEVELOPMENT OF INTERVENTRICULAR SEPTUM & PARTITION OF PRIMITIVE VENTRICLES
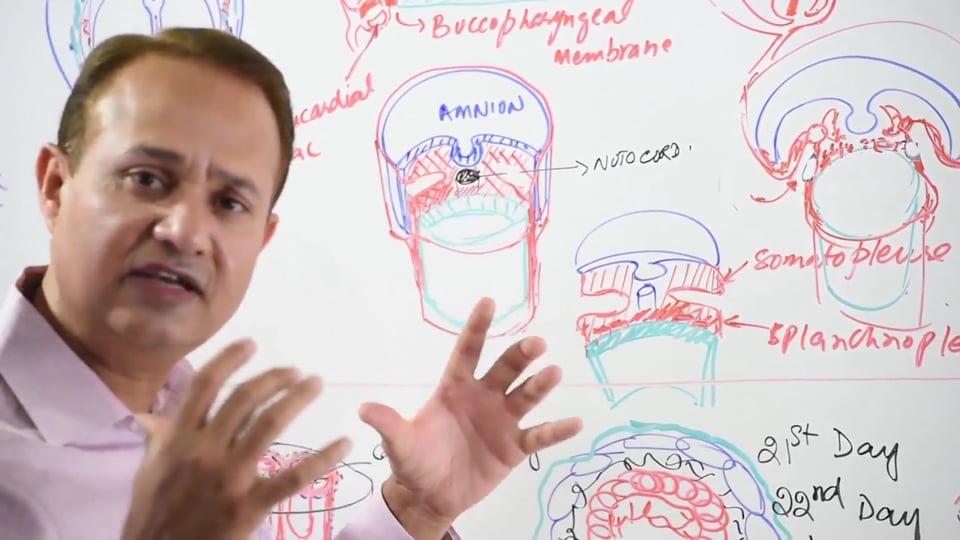
Embryonic time line of IV SEPTUM DEVELOPMENT: begins in the late 4th week and beginning of 5 th week. By the end of 4th week, the primitive ventricle is one single chamber which receives blood from the atria via the divided atrioventricular canal. Then there's also a single aorticopulmonary trunk opening into primitive ventricles which forms the outflow tract. At this point aorticopulmonary trunk is formed of bulbus cordis and truncus arteriosus and it provides the outflow tract for the primitive ventricles. During later parts of the development the bulbus cordis gets incorporated into the right and left ventricles. Upon incorporation, on the right side the bulbus cordis forms the infundibulum of the right ventricle, and on the left side it forms the vestibule of the left ventricle. Hence, bulbus cordis forms the smooth outflow tracts of the ventricles on either side. Truncus arteriosus on the other hand develops into forming aorta and the pulmonary trunk on the left and the right sides respectively.
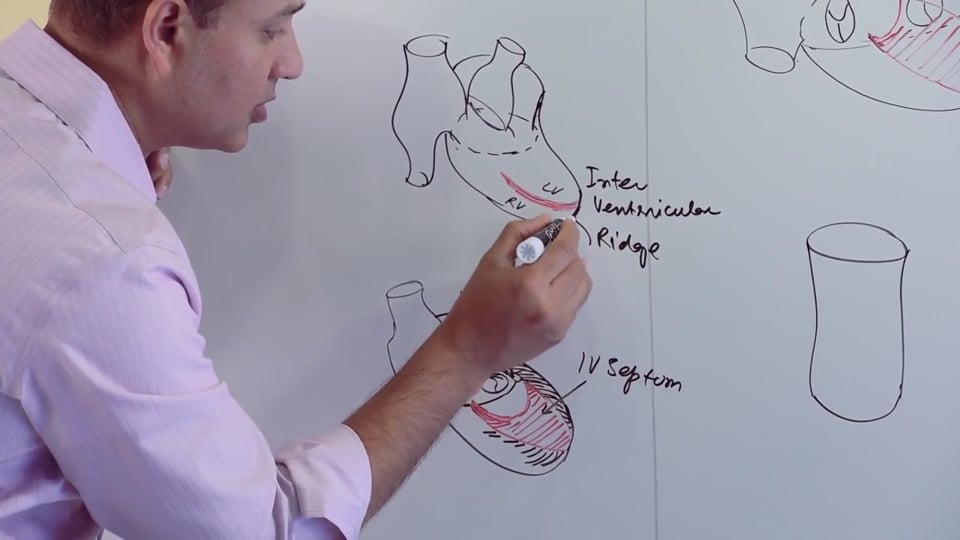
Adult IV septum consists of two parts, a muscular part (derived from the myocardial cells) which forms the majority of the septum, and a relatively thin membranous part which forms the superior aspect of the IV septum which is part of the outflow tract.
By the early 5th week, the muscular IV septum develops as an IV septal ridge from the floor of the primitive ventricle near the apex of the heart. This interventricular septal ridge ascends towards the atrioventricular canal, and thereby partially divides the primitive ventricle into left and right ventricles. The IV septal ridge extends towards the atrioventricular canal but it does not reach it, hence giving rise to a gap or defect which is referred to as interventricular foramen (IV Foramen). Thus the IV foramen is formed by the concave upper edge of the IV septum which gives rise to a gap through which shunting of blood between the right and left ventricles occurs.
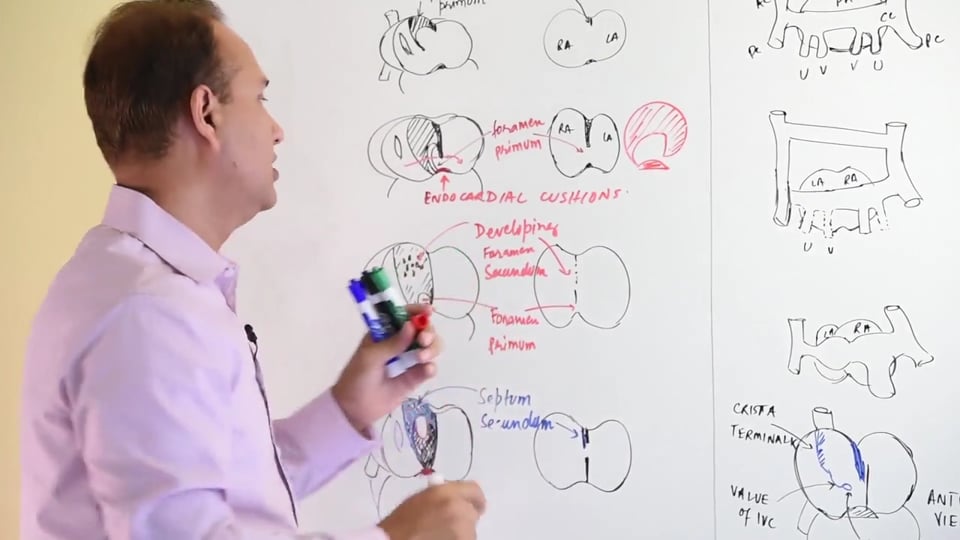
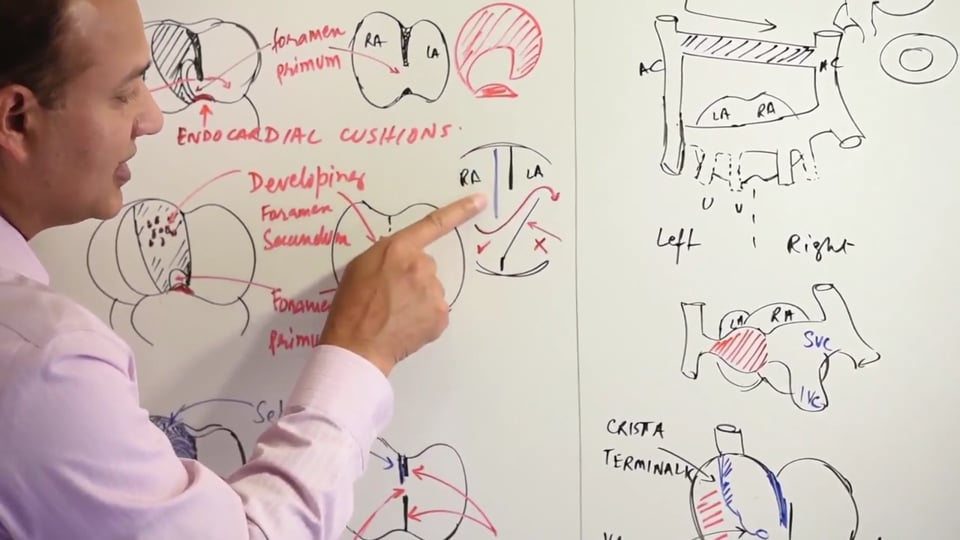
The membranous IV septum descends downward from the AV canal and fuses with the muscular IV septum thereby completely obliterating the IV foramen. The membranous part of IV septum is contributed by the following:
- Endocardial cushions (Neural crest cells derivative)
- Aorticopulmonary trunk septum (neural crest cell derivative)
- Muscular IV septum (Myocardial cells derivative)
CLINICAL DISORDERS ASSOCIATED WITH INTERVENTRICULAR SEPTUM DEVELOPMENT
- COR TRILOCULARE BIATRIUM: It's a three chambered heart with a single/common primitive ventricle and two atria. It occurs due to failure of development of the interventricular septum.
- MUSCULAR IV SEPTAL DEFECTS: During its development the muscular IV septum can present with defects or holes allowing left to right shunts. Severity of these defects depends upon the size of these gaps. The resultant shunting caused by these defects can lead to right ventricular hypertrophy.
- MEMBRANOUS IV SEPTAL DEFECTS: This is the most common of the IV septal defects. Part of the membranous IV septum is derived from the endocardial cushions which themselves are neural crest cells derivatives. Neural crest cells are also involved in the craniofacial development, therefore, abnormal migration of neural crest cells will result in concurrent facial and cardiac defects (mostly septal defects & atrioventricular valve problems). As mentioned earlier that it's the membranous IV septum which is responsible for filling the gap formed by the IV foramen. If there is any defect in the formation of the membranous part of IV septum, the IV foramen will remain patent and left to right shunting of blood will occur. The severity of the left to right shunting due to IV septal defects depends upon the size of the defect. Clinically IV septal defects manifest themselves as following:
- Excessive fatigability upon exertion.
- A harsh holosystolic murmur, best audible at the left lower sternal border.
- EISENMENGER COMPLEX: Initially the left to right shunting of the blood via the VSD is noncyanotic because it’s the oxygenated left ventricular blood mixing with the deoxygenated right ventricular blood. However, if this left to right shunt is left uncorrected, the increased blood flow into the right side of the heart can lead to pulmonary hypertension due to increased blood flow to the lungs. With time, this pulmonary hypertension can cause pathologic remodeling of pulmonary vasculature. This remodeling involves marked proliferation of tunica intima & media of the muscular pulmonary arteries and arterioles. Ultimately, pulmonary vascular resistance and the compensatory right ventricular hypertrophy together reverse the initial direction of the shunt from "left to right" to "right to left". After birth, a right to left shunt is cyanotic, because the blood via the shunt is bypassing pulmonary gaseous exchange process and hence remains deoxygenated. Eisenmenger complex presents with late cyanosis, clubbing and polycythemia.
Other than with ventricular septal defects, Eisenmenger complex can also present along with atrial septal defects and patent ductus arteriosus. It's important to remember that post birth, right to left shunts result in early cyanosis. Whereas, "left to right" shunts result in late cyanosis. Children suffering from late cyanosis are referred to as blue kids in contrast to the newborns which present with cyanosis at birth and are referred to as blue babies.
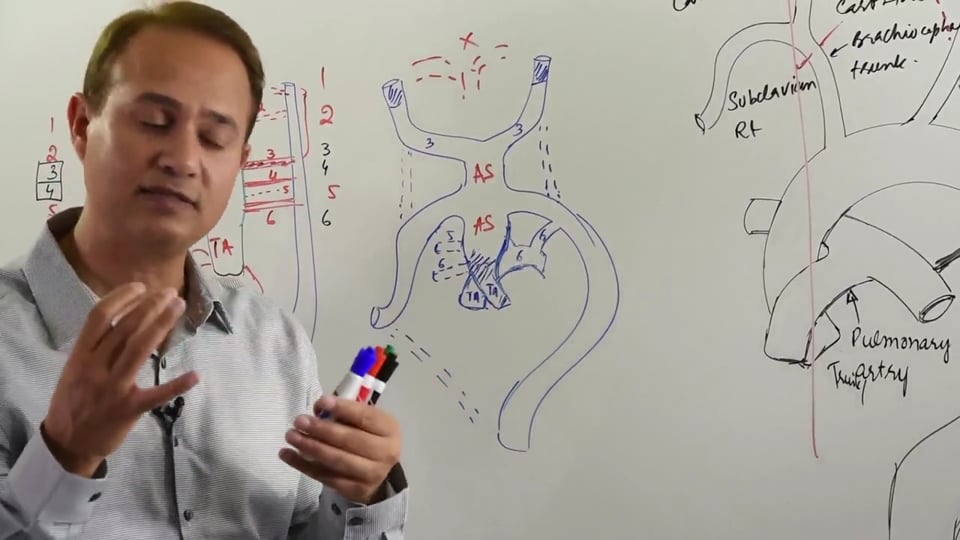
DEVELOPMENT OF AORTICOPULMONATY SEPTUM
Aorticopulmonary trunk arises from the primitive ventricles and serves as an outflow tract for the primitive ventricle. An aorticopulmonary septum forms within the aorticopulmonary trunk, thereby subsequently dividing it into the aorta & pulmonary trunk. Aorticopulmonary septum is formed by the migration of neural crest cells into the c conotruncal and bulbar ridges of the truncus arteriosus. These neural crest cells grow in a spiral fashion and fuse to form aorticopulmonary septum. As the aorticopulmonary septum descends as part of its growth, it spirals in such a fashion that aorta becomes the left ventricular outflow tract and the pulmonary trunk becomes the right ventricular outflow tract. As mentioned earlier, as part of its descent the aorticopulmonary septum contributes to the development of the membranous part of interventricular septum and therefore helps fill in the opening formed by the interventricular foramen.
DEFECTS IN THE DEVELOPMENT OF AORTICOPULMONARY SEPTUM result due to defects in migration of neural crest cells into the truncus arteriosus. At birth these aorticopulmonary septal defects always present with some cyanosis due to right to left shunting of the blood. Following are the congenital abnormalities associated with development of AP septum:
- PERSISTENT TRUNCUS ARTERIOSUS occurs when there's complete failure of the development of the AP septum due to abnormal migration of neural crest cells. As a result the separation of left ventricular and right ventricular outflow tracts never occurs. Therefore, the aorta and pulmonary trunk form a single outflow vessel (persistent truncus arteriosus) which receives blood from both the right and left ventricles. The common outflow tract allows mixing of oxygenated and deoxygenated blood, resulting in cyanosis of varying degree. Even though thetwo outflow tracts separate downstream, but by that time the mixing of oxygenated and deoxygenated blood has already occurred, hence it's a cyanotic defect. Persistent truncus arteriosus is always accompanied by a membranous VSD (AP septum contributes to the formation of membranous part of IV septum, only muscular IV septum forms)and therefore this further allows right to left shunting of the blood.
- TRANSPOSITION OF GREAT ARTERIES occurs when there's a failure of the AP septum to develop in a spiral fashion secondary to a defective migration of the neural crest cells. This results in a transposition of the outflow tracts, as a result of which, the left ventricle is connected to the pulmonary trunk and the right ventricle is connected to the aorta. Consequently, two completely closed non-communicating circuits are formed which involve the systemic and pulmonary circulations. The systemic circuit forms a closed loop carrying completely deoxygenated blood involving the right side of the heart and the aorta. The pulmonary circuit forms another closed loop carrying oxygenated blood, and involves the left side of the heart and the pulmonary trunk. As expected, transposition and resultant complete separation of pulmonary and systemic circulations lead to a situation which is incompatible with life in the absence of an accompanying shunt or mixing defects. Therefore, infants born alive with this defect tend to have other defects as well, which allow shunting and therefore mixing of oxygenated and deoxygenated bloods in between two otherwise closed circuits. As a result, for these newborns, accompanying shunting disorders (ASD, VSD, PDA, PFO)* are rather protective. Absence of a mixing defect requires an atrial septoplasty surgery to create a shunt so that mixing of could occur and thereby sustain life. Transposition of outflow tracts is the most common cause of severe cyanosis, which occurs and persists immediately after birth. Without any surgical intervention or maintenance of PDA (Prostaglandin E analogue administration), most infants don't survive past the first few months. It's important to remember that upon imaging, in case of great vessels transposition, the echocardiogram shows an aorta which lies anteriorly and to the right of the pulmonary artery.
- TETRALOGY OF FALLOT (ToF) is the most common of cyanotic congenital heart defect. This is caused by a misalignment of the aorticopulmonary septum, where it fails to divide the aorticopulmonary trunk in the midline. In case of ToF the AP septum is displaced anteriorly and towards the right or pulmonary side. This results in forming two unequal sized outflow vessels, with a very stenosed pulmonary artery and larger than normal aorta. As the name suggests, Tetralogy of Fallot has 4 component defects which coexist simultaneously. These 4 defects which as following (best remembered with mnemonic PROVe):
- Pulmonary Stenosis: it's a direct manifestation of the defective rightward misalignment of the AP septum.
- Overriding/Straddling Aorta: larger than normal calibre aorta which receives blood from both the left and right ventricles.
- Ventricular Septal defect: failure of AP septum to form the membranous part of the IV septum and subsequently fuse with the muscular IV septum, hence the IV foramen isn't closed which gives rise to a VSD.
- Right Ventricular Hypertrophy: develops secondary to pulmonary stenosis, because right ventricle has to pump against a greater resistance of a stenosed outflow tract thereby resulting in compensatory hypertrophy of the right ventricle.
Due to the presence of a ventricular septal defect, and a stenosed pulmonary outflow tract which presents with greater resistance to blood flow, there's a right to left shunting of the blood. This right to left shunting results in cyanosis because the blood leaving the heart via the aorta is mixed with deoxygenated blood from the right ventricle. A very important point to remember and which is highly tested as well is that, squatting tends to improve this cyanosis. This is because squatting tends to increase systemic vascular resistance or afterload, which tends to decrease right to left shunting of the blood via the VSD and thereby helps improve the cyanosis.
Clinically, ToF presents with a harsh systolic ejection murmur which can be auscultated at middle to left sternal border. This murmur occurs due to presence of right ventricular outflow tract obstruction.
KEY:
ASD= Atrial septal defect
VSD= Ventricular septal defect
PDA= Patent ductus arteriosus
PFO= Persistent foramen ovale
AP= Aorticopulmonary
IV= Interventricular
In this video we will learn about :
1. Development of inter ventricular septum.
2. Development of aorticopulmonary septum.
3. Patent truncus arteriosus.
4. Transposition of great vessels.
5. Tetrology of fallot.











Write A New Comment
0 Comments