This video presents nodal action potentials. These action potentials occur in the cardiac tissues that exhibit automaticity. A comparison of the myocardial action potential with the nodal action potential is also made to make sure that you are not confused during the Steps.
STUDY NOTES:
NODAL ACTION POTENTIAL
NODAL ACTION POTENTIAL VS. VENTRICULAR ACTION POTENTIAL
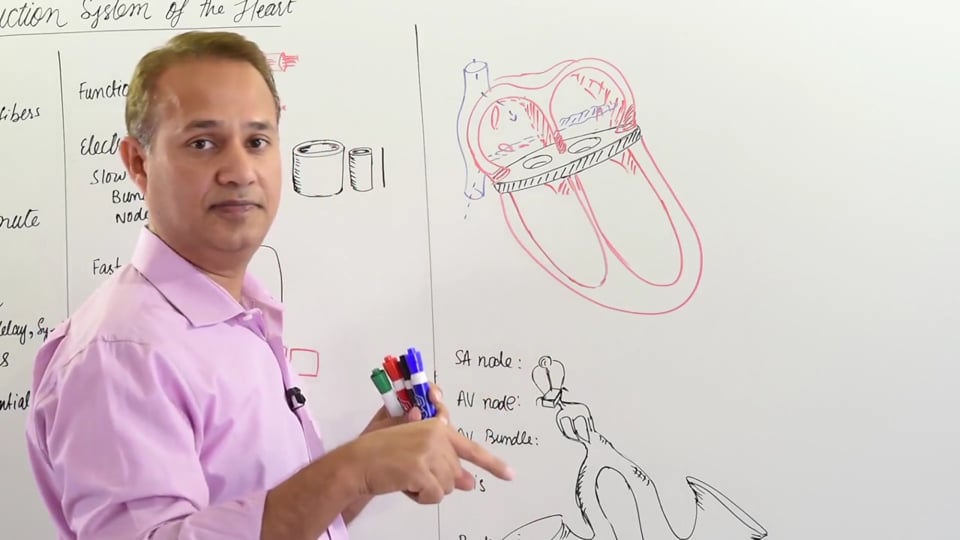
The nodal tissues and the Purkinje fibers exhibit automaticity in their properties as they are able to undergo spontaneous depolarizations. In other words, these tissues do not require the need of an external stimulus or a trigger to undergo depolarization. This is in contrast to ventricular fibers that do not show automaticity. The reason behind this phenomenon can be explained as follow:
• The resting membrane potential (RMP) of nodal tissues is less negative than the RMP of ventricular fibers. This allows the nodal tissue channels to operate in a semi-activated state even during the resting phase of the action potential. The comparatively more negative ventricular fibers do not show this property and hence, are not easily activated by low voltage impulses.
• Secondly, the presence of fast sodium channels and slow calcium channels, in ventricular fibers and nodal tissue respectively, play an important role in the automaticity of a cell. The slow calcium channels in the nodal tissues are responsible for the peak voltage occurring during a nodal action potential. Whereas, in the ventricular muscle fibers, the fast sodium channels are responsible for the same voltage spike and the calcium channels are involved only during the plateau phase.
PHASES DURING AN ACTION POTENTIAL
|
PHASE OF ACTION POTENTIAL |
VENTRICULAR MUSCLE FIBER |
NODAL TISSUES |
|
Phase 0 |
Opening of Sodium channels (Depolarization) |
Opening of Calcium channels (Depolarization) |
|
Phase 1 |
Opening of transient Potassium & Chloride channels |
Does not occur |
|
Phase 2 |
Plateau phase: Opening of slow Calcium channels |
Does not occur |
|
Phase 3 |
Repolarization: Opening of Potassium channels |
Repolarization: Opening of Potassium channels |
|
Phase 4 |
Resting Membrane Potential |
Resting Membrane Potential |
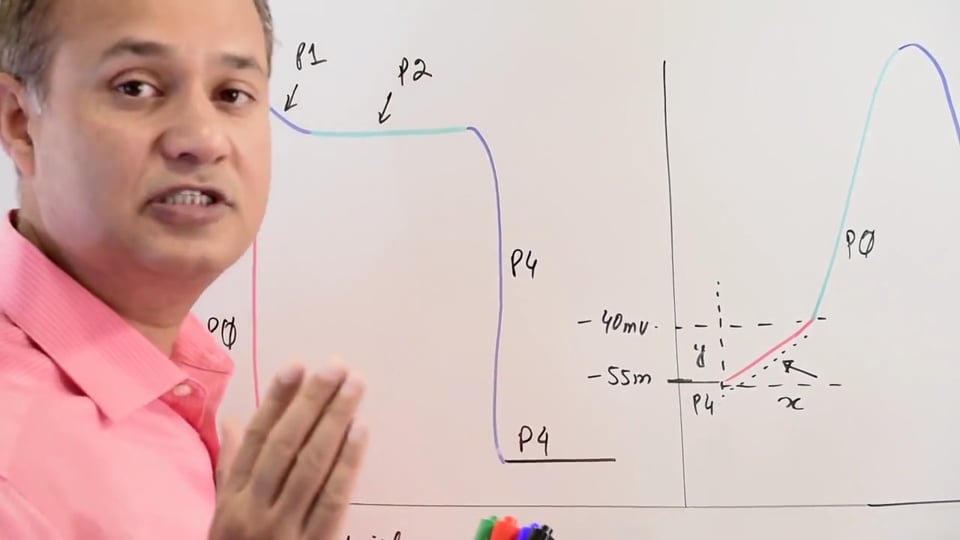
SLOPE OF DEPOLARIZATION DURING NODAL ACTION POTENTIAL
There is a gradual increase in the RMP of nodal tissues from -55mV to -40mV. This is known as the slope of depolarization, after which occurs the Phase 0 of action potential. This slope is important as multiple factors, such as the ANS and certain drugs, act to alter this phase and bring about changes in the rate and rhythm of cardiac activity. An increase in the slope of depolarization will cause the SA Nodeto generate action potentials at a higher rate. Flattening of the slope will result in fewer numbers of action potentials in a given time which greatly decreases the rate at which the heart beats.
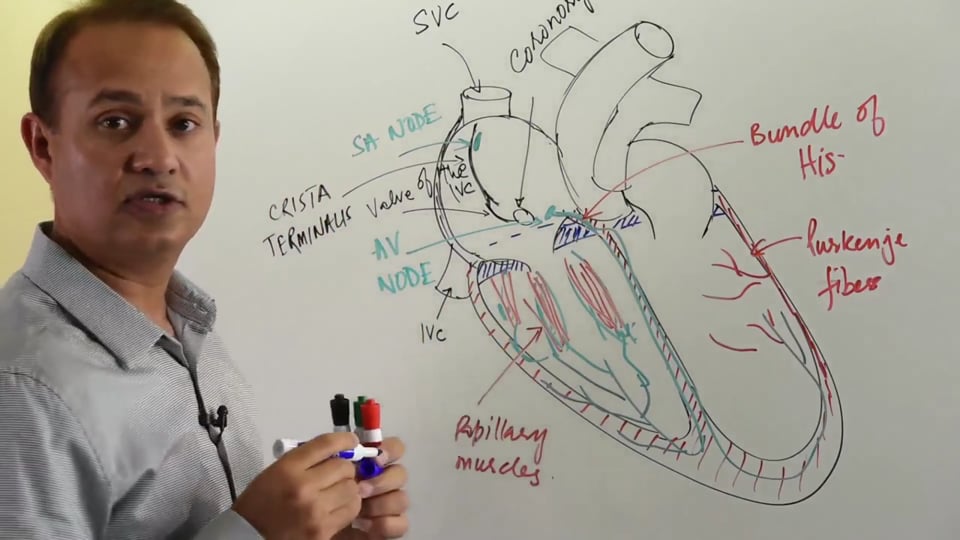
CONTROL OF HEART RATE & CONDUCTION VELOCITY
An isolated SA node has the highest intrinsic rhythm of impulse generation, i.e. 100 beats/min. This intrinsic rhythm of SA Node is regulated down to 72 beats/min under the influence of the autonomic nervous system. Similarly, the AV node has the ability to depolarize at a rate of 55 beats/min. SANode, having a considerably higher frequency of depolarization, overrides the pace maker activity of the AVNode. This causes the AV node to generate action potentials at a rate similar to SA node. Upon cessation of high frequency impulses from SA node, as happens during bundle blocks, the AV node is shown to beat at its own inherent frequency. Impulse generation of purkinje fibers is at a rate of 15-30 beats/min. There is a respective decrease in the frequency of depolarization as we move along the bundle of His and the Purkinje fibers. This relative difference in the intrinsic rhythm of different parts of the cardiac conduction system allows a uni-directional flow of impulses across the entire conducting system.
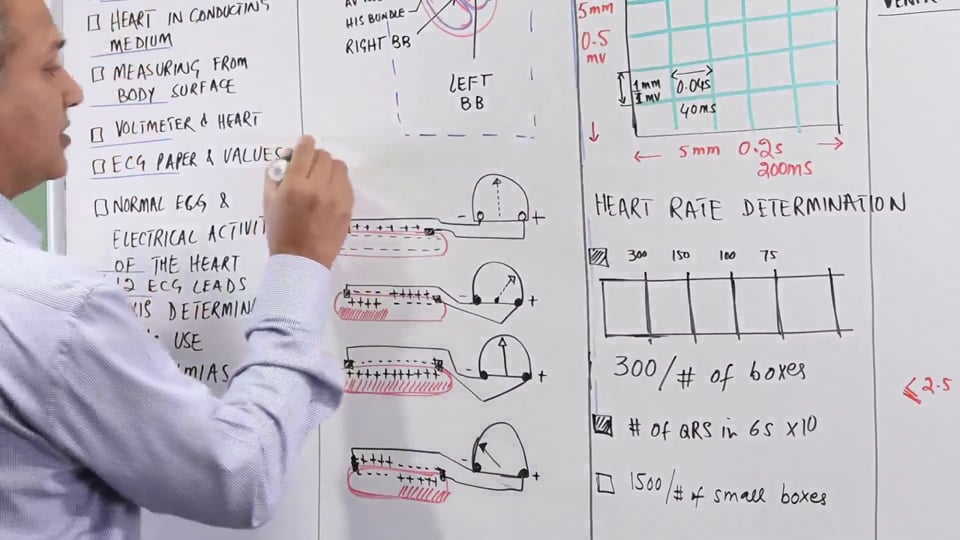
As described above, the SA node has the highest rate of depolarization and therefore, it dictates the rate of cardiac activity. Altering with the mechanics of SA node will cause alterations in the rate of heart beat as a whole. Similarly, the velocity of conduction is controlled by the AV node(dimensions are 1*3*5 mm) and AV bundles as the speed of impulse travelling through them is the slowest. Time duration for conduction through these is 0.12 seconds. Velocity of impulse at AV node and AV bundle is 2 meters per second and 4 meters per second in purkinje fibers. Dromotropes act on these areas of the conducting system and cause changes in the velocity of impulse conduction.
DIFFERENT ION CHANNELS AND THEIR AFFECT ON THE ACTION POTENTIAL
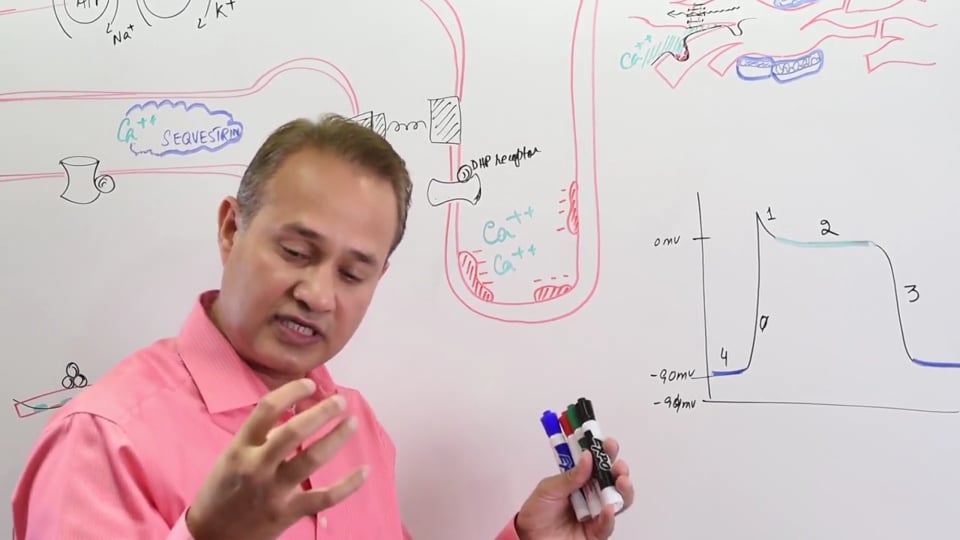
1) VENTRICULAR ACTION POTENTIAL
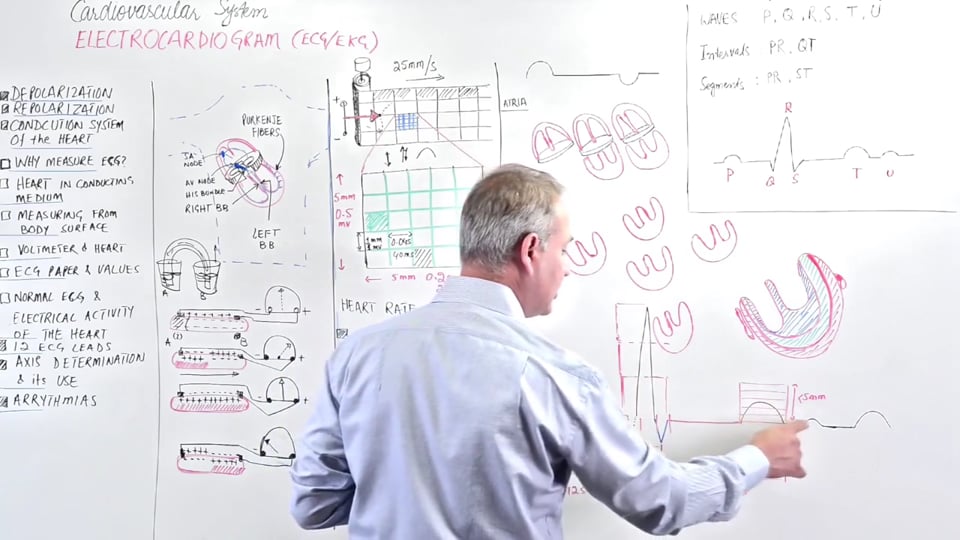
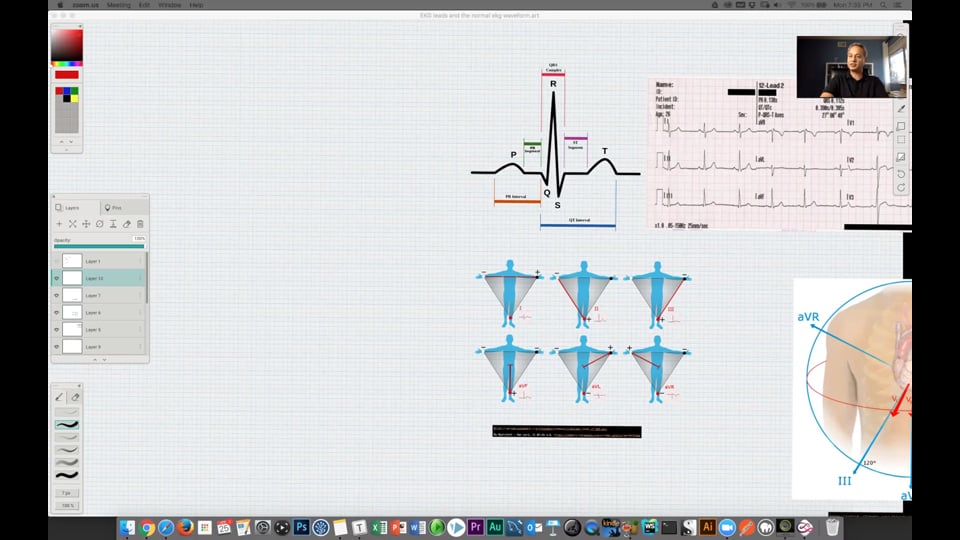
• The Phase 0 of ventricular action potential is brought about by fast voltage gated sodium channels. This phase is referred to as the upstroke of action potential and corresponds to the QRS complex of the ECG.
• At the end of depolarization, there is a brief fall in the voltage of action potential as a result of opening of transient chloride and potassium channels. This isPhase 1 of the depolarization. Fast sodium channels transition to their inactivated state.
• L-type Calcium channels open in the Phase 2 of action potential. The inward calcium current balances the outward potassium current and there’s little change in membrane potential, which explains the plateau. During this plateau phase no change in the voltage is registered. Phase 2 or the plateau phase of the ventricular action potential corresponds to ST segment of the ECG.
• Phase 3 corresponds to repolarization during which Potassium channels open in response to voltage and ion concentration difference. By this time L-type Calcium channels, which were open during the plateau phase, have also closed. Repolarization corresponds to the T-wave on the ECG. Inward Potassium current enters via the:
▪ IK1 channels: Inward rectifying K channel
▪ IKR channels: Slow and rapid delayed rectifying K channel
• The action potential is brought back to the resting membrane potential (RMP) or Phase 4. The sodium-potassium ATP-ase is responsible for the maintenance of RMP until the arrival of the next action potential. Fast Na+, L-type Ca2+, and rectifying K+ channels (IKR) close, but IK1 channels remain open.
2) NODAL ACTION POTENTIAL
It’s important to understand that the nodal tissue (SA and AV) lacks fast Na+ channels. Thus, the upstroke of the action potential is mediated by inward calcium current rather than the sodium current. In addition, note that phases 1 and 2 are absent in the nodal tissue.
• The RMP (Phase 4) in nodal tissue is kept at -55mV by the Na-K ATPase pump. The less negative RMP of nodal tissue, compared to -70mV of ventricular tissues, allows it to exhibit automaticity. At -55mV, the fast sodium channels (also known as 'funny' channels) are in a semi-open state which causes leakage of positive ions into the nodal cells. Leakage of ions causes an increase in the membrane potential in a positive direction. The membrane potential gradually increases to -40mV. Upon reaching this threshold potential, the sodium channels close and remain closed for the rest of the action potential as they enter a state of refractoriness.
• At this point the slow-gated T-type calcium channels open which creates the spike of depolarization (Phase 0). These differ from the L-type calcium channels (in the ventricular tissue) in that they open at a more negative membrane potential (-70 mV).The calcium ions that enter the cells during this phase are also involved in excitation-contraction coupling of the myosin light chains with actin filaments.
• Repolarization (Phase 3) in nodal tissue is similar to that of ventricular muscle fibers. Inward Potassium current enters via the IK1 & IKR (rectifying K currents) channels. The fall in membrane potential will result in activation of the sodium-potassium ATPase and the cycle is repeated.
In this video we will learn about:
1. Nodal vs. ventricular action potential.
2. Phases of nodal action potential.
3. Control of the heart rate and conduction velocity.
4. Channels involved in generating nodal action potential.
5. Automaticity or self excitation.
Presented by Dr. Mobeen Syed


Write A New Comment
1 Comments
elbarchouroucke@*.com
Sep 12 2023, 10:51 am
Nodal tissu doesn't include his bundle and av bundle?