Hyponatremia
Duration: 1:05:55
Published On Jun 2, 2017
In this lecture, we review sodium homeostasis in the human body as well as hyponatremia. Critical care management of hyponatremia is discussed. The differential diagnosis of hyponatremia will be outlined and an approach to its etiology is reviewed.
Learning objectives of this video are the following:
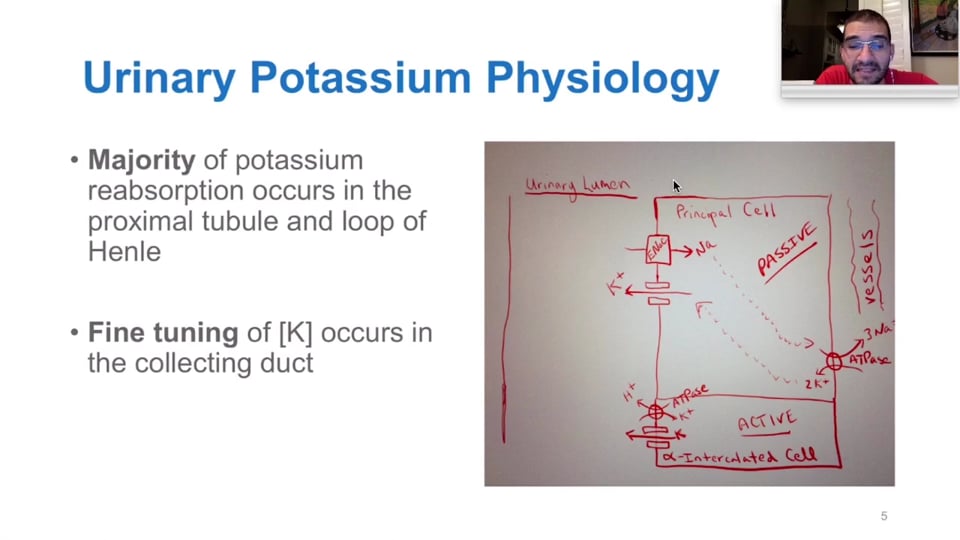
1. Review of sodium homeostasis in the human body.
2. Hyponatremia.
3. General causes of hyponatremia.
4. Emergent management of hyponatremia.
5. Differential diagnosis.
6. Clinical uses.
Presented by Dr. Luis A Verduzco
Following answers are created by ChatGPT. Occasionally the answer may be harmful, incorrect, false, misleading, incomplete, or limited in knowledge of world. Please contact your doctor for all healthcare decisions. Also, double check the answer provided by the AI below.
Faculty
In addition to the presenter, following authors may have helped with the content writing, review, or approval:
CME, CE, CEU and Other Credit Types:
ACCME Accreditation Statement
The DrBeen Corp is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to
provide continuing medical education for physicians.
AMA Credit Designation Statement
The DrBeen Corp designates this enduring material for a maximum of 1.25 AMA PRA Category 1
Credits™.
Physicians should claim only the credit commensurate with the extent of their participation in the
activity.
Disclosure Information
In accordance with the disclosure policies of DrBeen Corp and the ACCME (Accreditation Council for
Continuing Medical Education), we are committed to upholding principles of balance, independence,
objectivity, and scientific rigor in all of our Continuing Medical Education (CME) and Continuing
Education (CE) activities. These policies include the careful management and mitigation of any relevant
financial relationships with organizations that are not eligible.
All members of the Activity Planning Committee and presenters have disclosed their relevant financial
relationships. The DrBeen Corp CE Committee has thoroughly reviewed these disclosures and determined
that these relationships are not deemed inappropriate in the context of their respective presentations.
Additionally, they are found to be consistent with the educational objectives and the integrity of the
activity.
| Faculty | Disclosures |
|---|---|
| Author declares no conflict of interest. |
Instructors
Intensive Care Unit (ICU/CCU)

ICU Module
05:18
Luis A Verduzco M.D.
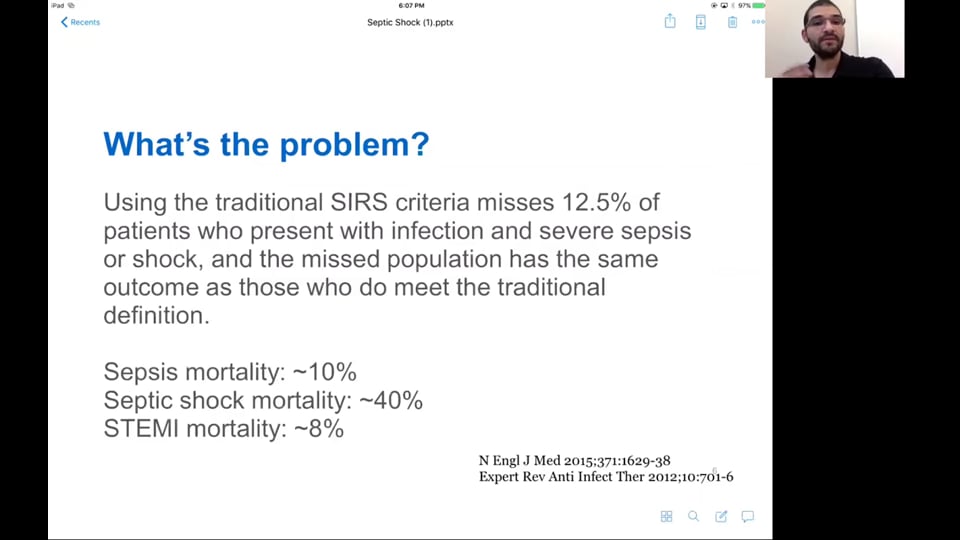
A Preview of Sepsis and Septic Shock: Diagnosis and Management
01:44
Luis A Verduzco M.D.
 0.50 CME
0.50 CME
Management of Brain Trauma (Part 1)
30:26
Luis A Verduzco M.D.
 0.50 CME
0.50 CME
Management of Brain Trauma (Part 2)
36:09
Luis A Verduzco M.D.
 0.75 CME
0.75 CME
Hyperkalemia and Its Management
46:09
Luis A Verduzco M.D.
 1.75 CME
1.75 CME
Management and Diagnosis of Sepsis and Septic Shock
1:41:46
Luis A Verduzco M.D.
 0.75 CME
0.75 CME
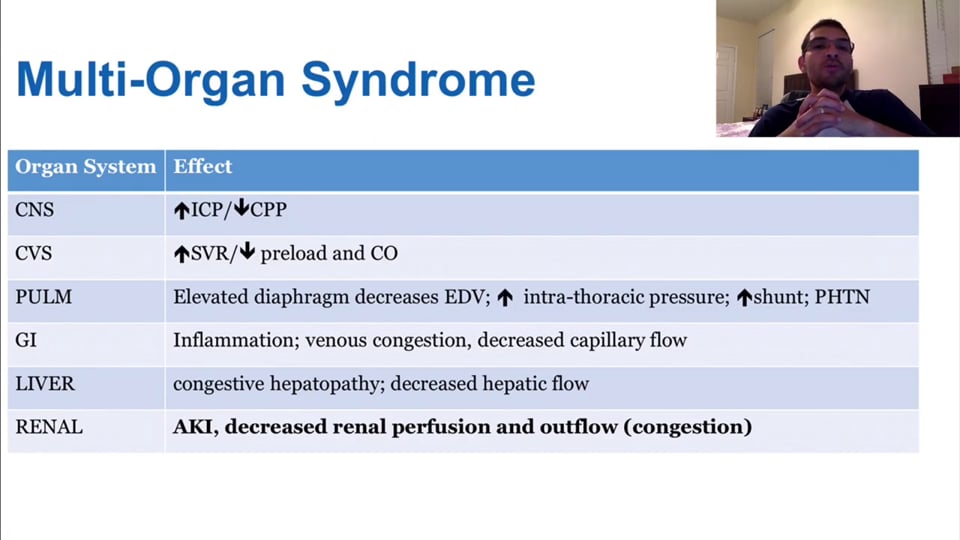
Abdominal Compartment Syndrome
51:15
Luis A Verduzco M.D.
1.00 CME
Hyponatremia
1:05:55
Luis A Verduzco M.D.

Cardiac Drugs: Inotropes, Vasopressors, and Vasodilators Part 1
33:33
Luis A Verduzco M.D.
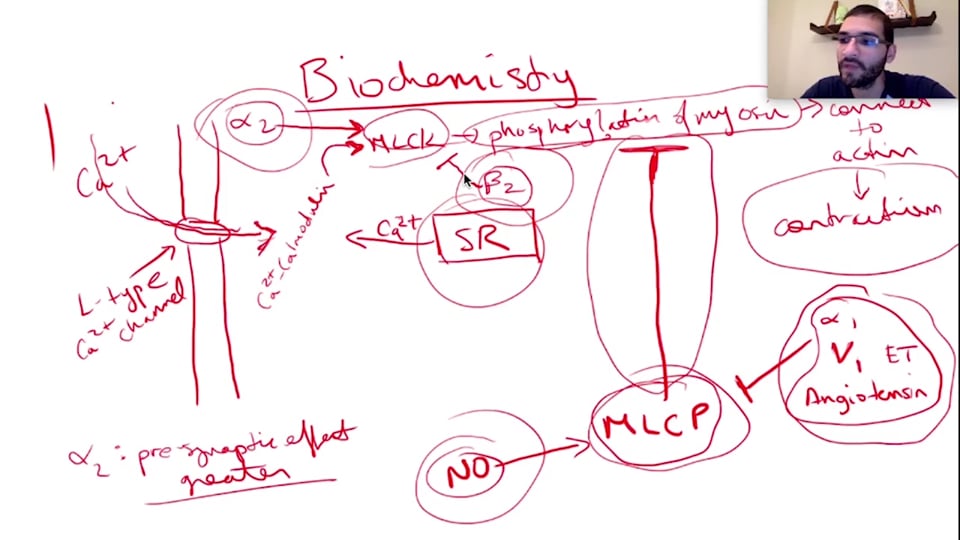
Cardiac Drugs: Inotropes, Vasopressors, and Vasodilators Part 2
48:59
Luis A Verduzco M.D.
 1.50 CME
1.50 CME
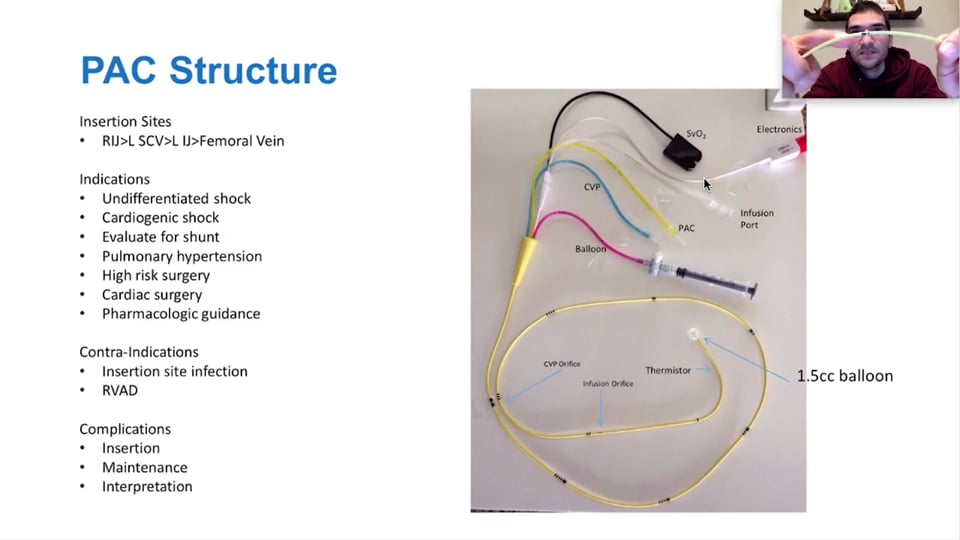
PA Catheter
1:30:17
Luis A Verduzco M.D.
 1.25 CME
1.25 CME
Perioperative Cardiac Complications
1:07:43
Luis A Verduzco M.D.
 0.75 CME
0.75 CME
Sedation and Analgesia
51:09
Luis A Verduzco M.D.
 1.00 CME
1.00 CME
Diagnosis and Management of Chronic Obstructive Pulmonary Disease (COPD)
1:06:31
Luis A Verduzco M.D.
 1.25 CME
1.25 CME
Medical Fallacies
1:13:51
Luis A Verduzco M.D.

Coma: Definition, Etiologies, and a Case for Review
36:41
Ana Crawford M.D., M.Sc.
 0.75 CME
0.75 CME
Webinar - Glasgow Coma Scale - Examination of a Patient in Coma
48:28
Dr. Mobeen Syed
 0.05 CME
0.05 CME
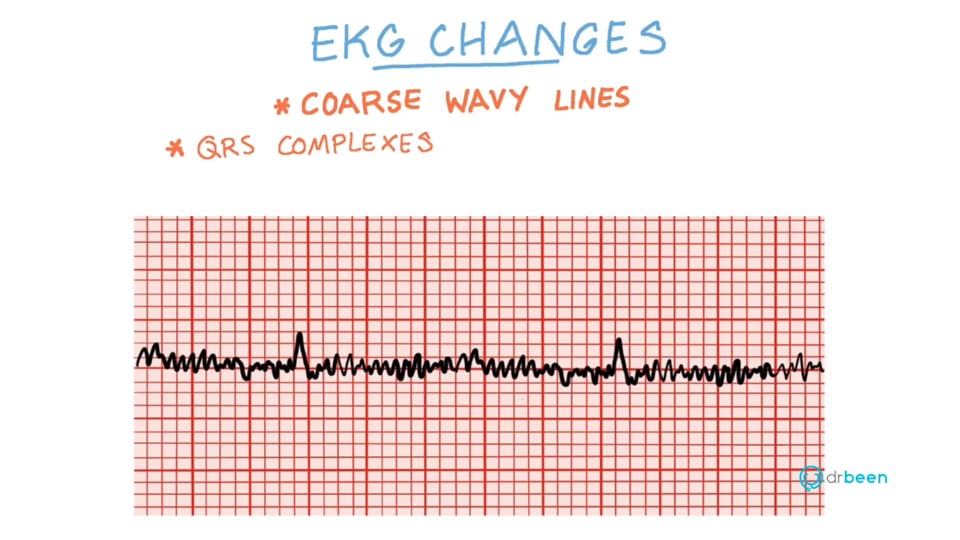
Ventricular Fibrillation (V-Fib)
03:13
Dr. Mobeen Syed
 0.75 CME
0.75 CME
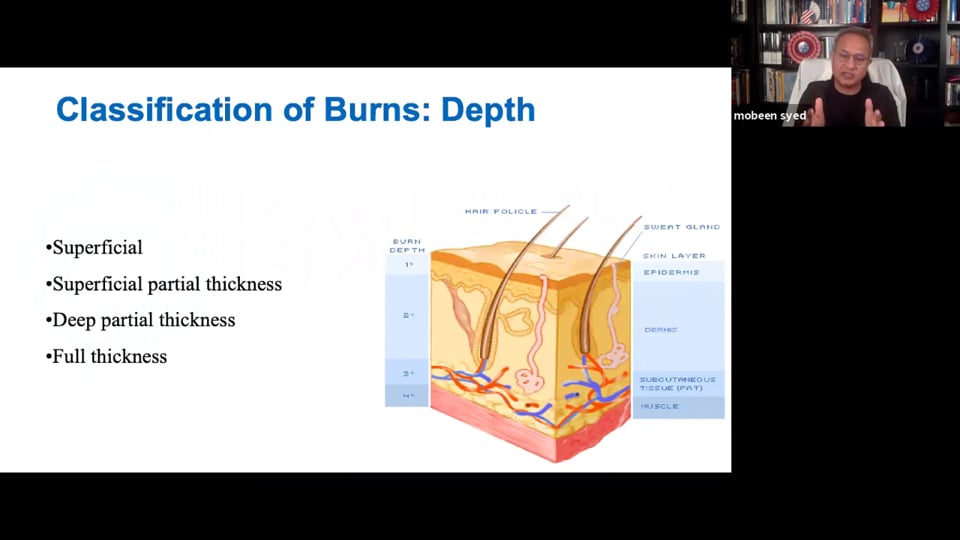
Basic Assessment and Management of Burns
43:47
Zeshaan Maan MD
Dr. Mobeen Syed
 0.50 CME
0.50 CME
Burns Questions and Answers with Dr. Zeshaan Maan
28:54
Zeshaan Maan MD
 0.75 CME
0.75 CME
Burns: A comprehensive look at burn pathophysiology and clinical management
47:47
Ahmed Zaafran, MD
Write A New Comment
2 Comments
toyangmd@*.com
Apr 05 2024, 8:33 pm
Anatomy
mjlthayer@*.com
Mar 02 2023, 8:17 pm
Great lecture