Atrial & Ventricular septum formation process begins at the same time by the start of the 4th week and wraps up by the 8th week. Though occurring simultaneously, however, atrial septation is a little ahead of ventricular septation. Common congenital cardiac anomalies mostly occur due to defects in the formation of these septae. In this lecture and its subsequent review, we discuss the high yield topic of atrial septation and development plus relevant congenital defect which can occur during this process.
FUNCTION OF INTERATRIAL SPETUM:
-
It divides the primitive atria into a right and left atria.
-
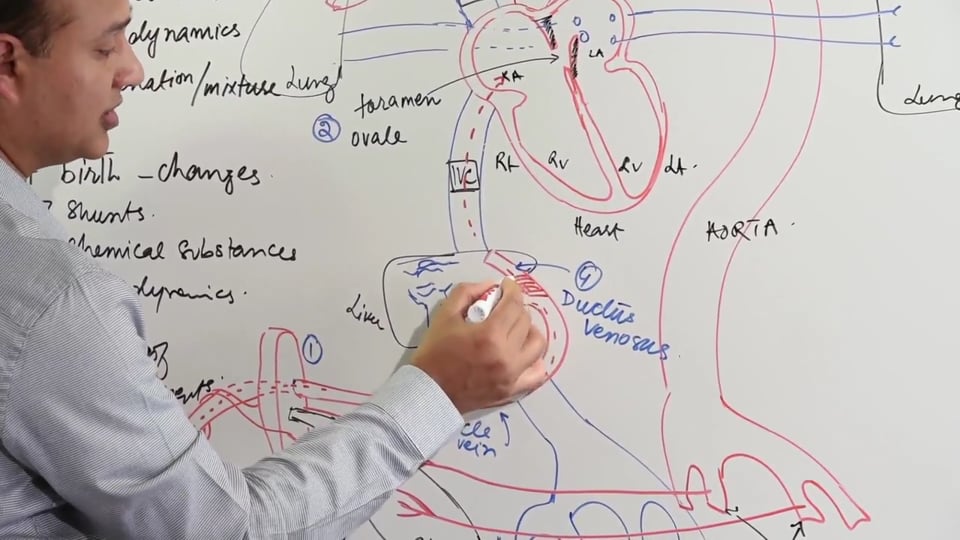
During fetal life provides it provides a patent right to left shunt and ensures the shunt is not in the opposite direction of left to right shunt. During fetal life right to left shunts are essential for the survival of the fetus. A hallmark of the fetal circulation, which differentiates it from the adult circulation, is that the right atrium receives the oxygenated blood from the placenta via the inferior vena cava. In an adult heart, the right side deals with the deoxygenated blood!
-
After birth, when there's no need a right to left shunt since the lungs have become functional, foramen ovale tends to close. At this point interatrial septum divides adult left and right atria into separate non-communicating chambers.
ATRIAL SEPTATION:
Embryonic timeline of Atrial Septation: Late 4th week to the middle of the 6th week.
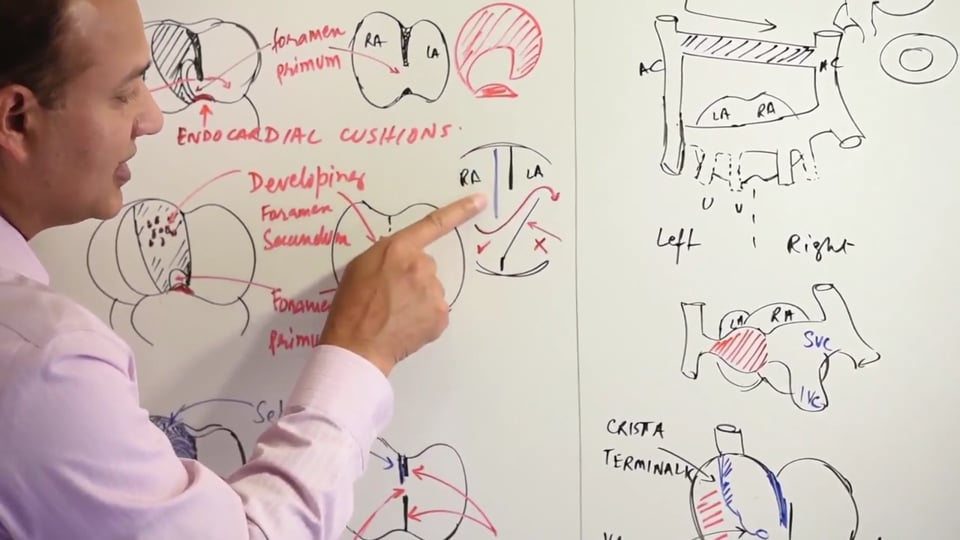
Initially the right and the left atria are actually one single chamber which is referred to Primitive Atrium. Sinus Venosus provides the Inflow in this primitive atrium. The primitive atrium is divided into two separate left and right atria following the process of atrial septation. Atrial Septation is actually a series of events which involves 2 septae (Septum Primum & Septum Secundum) and 2 foraminae (Foramen Primum & Foramen Secundum) forming within the primitive atria, thereby dividing it into a right and left atrium.
STEPS INVOLVED IN ATRIAL SEPTATION:
-
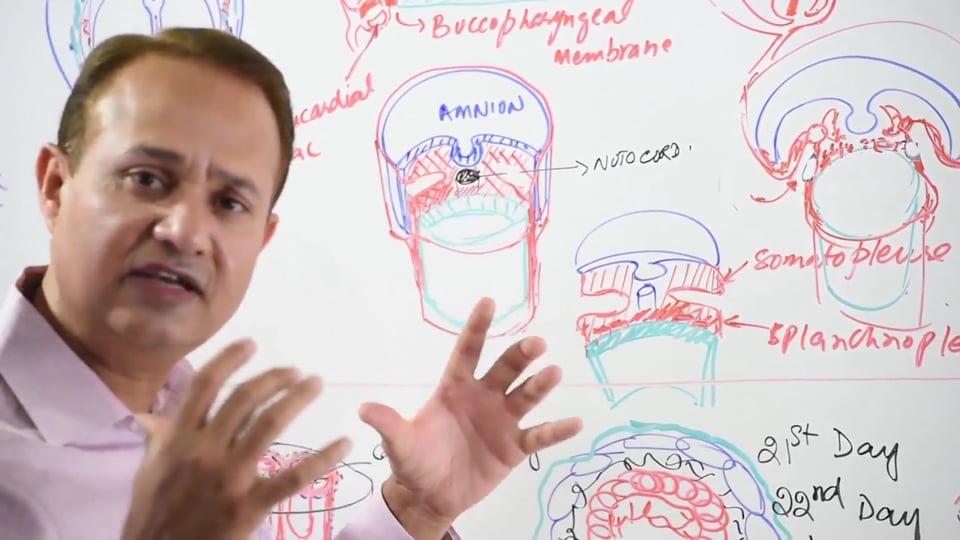
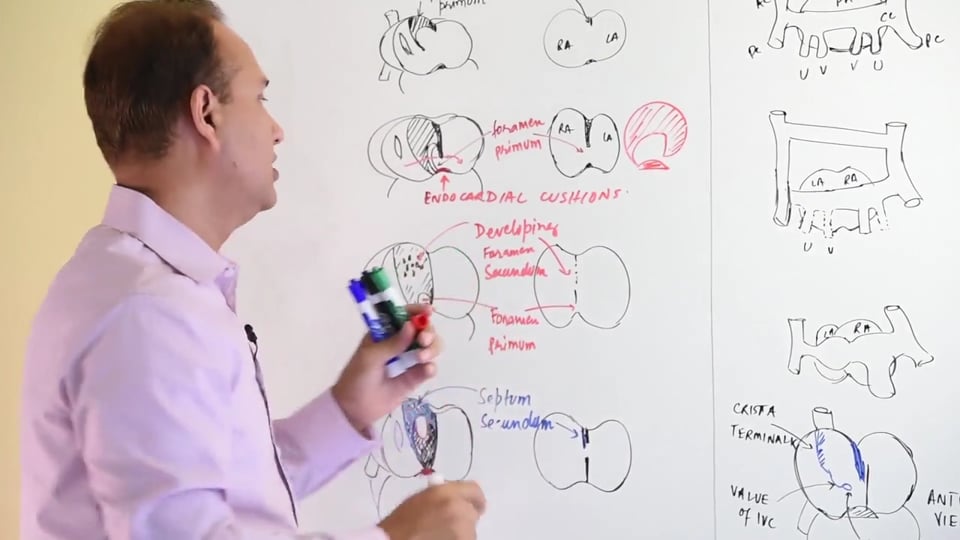
From the roof of the primitive atrium a flexible and crescenteric shaped Septum Primum grows inferiorly towards the endocardial cushions. The initial defect in between the down growing septum primum and the endocardial cushions is referred to as foramen primum. Foramen Primum functions to allow shunting of blood from the right atrium to the left atrium. Endocardial cushion itself is a derivative of neural crest cells and gives rise to the following structures in a adult heart:
- Atrioventricular Valves
-
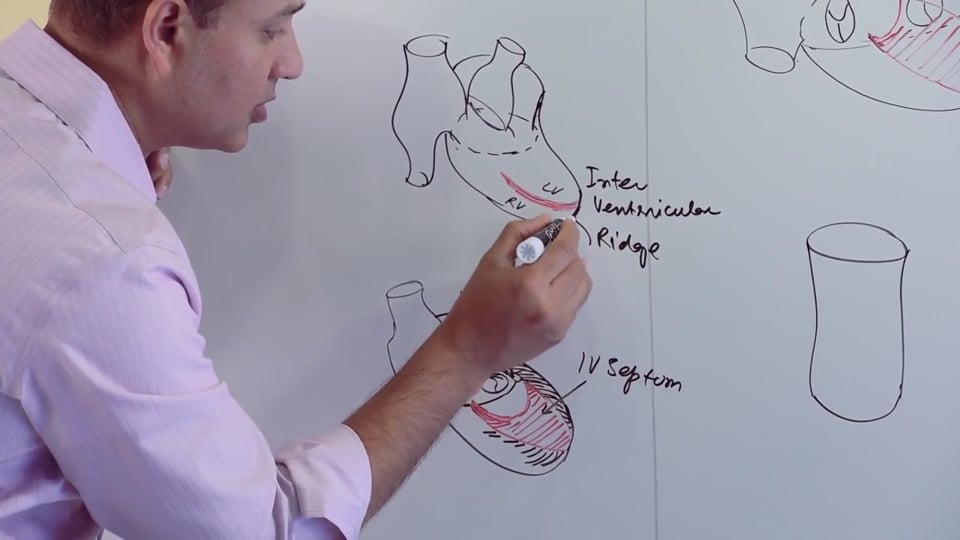
Membranous part of Interventricular septum
-
Aorticopulmonary septum
-
Left & Right Atrioventricular canals
-
Foramen Primum is eventually obliterated when the inferior edge of the septum primum fuses with the endocardial cushions. Just before the foramen primum closes, multiple small secondary defects form within the upper wall of septum primum as result of apoptosis. These multiple small defects in the upper wall of septum primum coalesce into forming a single defect called the foramen secundum. Foramen secundum is formed before the foramen primum is closed, and it serves to maintain the very important function of reinforcing a right to left shunt of the oxygenated blood entering the right atrium via the inferior vena cava.
-
While the septum primum is undergoing these changes, from the roof of the atrium and just to the right of septum primum, a second crescentic shaped septum secundum starts developing. As the septum secundum grows downwards, it extends and obliterates most of the foramen secundum. The remaining part of foramen secundum which isn't obliterated by the septum secundum is referred to as Foramen Ovale. The function of foramen ovale is the same as that of the foraminae primum and secundum, which was to maintain a right to left shunt.
-
It's important to remember that septum primum is a rather flexible structure compared to septum secundum which is a relatively rigid structure. This rather flexible property of the septum primum allows its inferior flap (which isn't covered by the septum secundum) to function as valve for foramen ovale. This valve allows the flow of blood from the right to left side thereby reinforcing the shunt, but it tends to disallow the backflow of the blood from the left atria to the right atria.
-
Septum Primum and Septum Secundum eventually fuse to form the interatrial septum. Most of the interatrial septum is formed from two septae (primum and secundum). However, the inferior part of the interatrial septum forms from a single septum (septum primum only), and hence this part is rather thinner compared to the rest of the atrial septae. This thinner part of the interatrial septum in the adult heart is referred to as Fossa Ovalis and is a major anatomical landmark of the adult right atrium. Fossa ovalis presents as a marked crescentic ridge on the medial wall of the right atrium.
-
Immediately after birth Foramen Ovale tends to close. After birth there's an increase in left atrial pressure due to decreased pulmonary vascular resistance which enhances pulmonary blood flow and subsequent return of blood to the left side of the heart. Also, closure of the umbilical veins tends to decrease the right atrial pressure with respect to left atrial pressure. The above mentioned decreased right atrial and increased left atrial pressure changes result in closure of the foramen ovale after birth.
CLINICAL & PATHOLOGICAL CONSIDERATIONS:
-
PROBE PATENCY OF FORAMEN OVALE: A probe is passed from the right atrium into the left atrium to check whether the foramen ovale has closed or not. In cases where the probe can pass through into the left atrium, it means that septum secundum & septum primum have not fused completely together and hence the foramen ovale is still patent. Patent foramen ovale is present in 25% of normal adults without any symptoms. Even if it's patent, the foramen ovale remains functionally closed due to post birth increased left atrial pressure. However, transient increase in right atrial pressure above the left atrial pressure (such as during Valsalva manoeuvre) can lead to a right to left shunt via the patent foramen ovale. This can lead to paradoxical emboli, where venous thromboemboli cross into the systemic arterial circulation and can cause various clinical complications.
-
FORAMEN SECUNDUM DEFECT/ SECUNDUM TYPE ASD: This is the most common type of ASD, which usually presents with delayed clinical symptoms after the age of 30, before the age of 30 it's usually asymptomatic. Secundum type ASD presents with variable sized defects in between the right and left atria. These defects are present in the central part of the interatrial septum, just above the limbus. Secundum type defects may occur due to one of the following, or both:
- Excessive resorption of the Septum Primum can result in a very large Foramen Secundum being formed which couldn't be effectively closed by the Septum Secundum.
- Alternatively Secundum type defects can occur when there's an underdeveloped septum secundum which has a relatively smaller size and hence cannot efficiently obliterate the foramen ovale.
Besides Secundum type defects, although much less common but there are also Primum type atrial septal defects. These primum type atrial septal defects result due to a failure of the septum primum to fuse inferiorly with the endocardial cushions. These Primum type defects can be located in the lower aspect of interatrial septum. Fossa ovalis tends to normal in primum type defects.
Clinical signs of atrial septal defects include:
- Wide, fixed splitting of S2.
- Systolic ejection murmur best audible in the 2nd intercostals space along the left sternal border.
- Atrial septal defects can also lead to paradoxical emboli similar to those in case of patent foramen ovale.
- COR TRICLOCULARE BI VENTRICULARE: It's basically a three chambered heart with one common atrium and two ventricles, thereby highlighting the situation where interatrial septum fails to develop.
-
PREMATURE CLOSURE OF THE FORAMEN OVALE: As mentioned earlier that foramen ovale is supposed to remain patent until after birth. If however, foramen ovale closes early due to premature fusion of septae primum & secundum before birth, this can result in a hypertrophied right and left ventricles plus an underdeveloped left sided chambers.
DEVELOPMENT OF RIGHT ATRIUM & THE FATE OF SINUS VENOSUS:
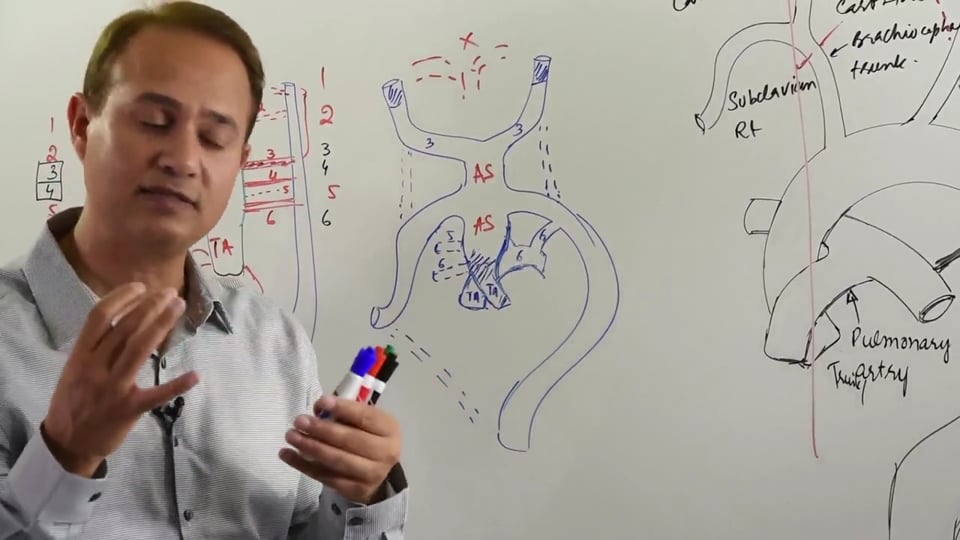
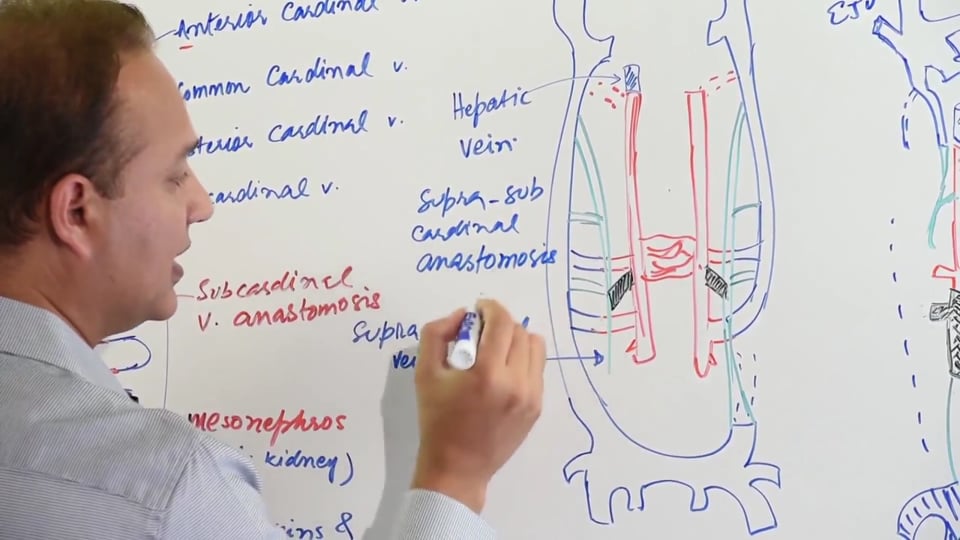
Heart tube with its dilatations undergoes an S-shaped bending which results in an orientation where the outflow tract (truncus arteriosus) lies most anteriorly. Behind the truncus arteriosus is the primitive ventricle and still behind is the primitive atrium. On the posterior surface of the primitive atrium opens the sinus venosus along with its branches. Branches of sinus venosus are anterior cardinal vein, posterior cardinal vein and the common cardinal vein. Two vitelline and umbilical veins also drain into sinus venosus. Initially the sinus venosus drains into the middle of the posterior wall of right atrium, however due to flow and hemodynamic changes, sinus venosus starts growing towards the right side. Ultimately sinus venosus ends up opening at the posterior right end of the right atrium. Hemodynamic changes responsible for this right side shifting of sinus venosus are as following:
-
An anastomosis forms between the anterior cardinal veins of either side, and the blood starts flowing from the left to the right side.
-
Umbilical and vitelline veins on the left side start degenerating. This results in an increased blood flow into the right side as blood from the caudal part of the fetus is also shunted to the right side of the right atrium.
-
Eventually the right umbilical vein also degenerates, and the right vitelline vein starts increasing in calibre. End result of these hemodynamic changes is that sinus venosus shifts and starts growing on the right side.
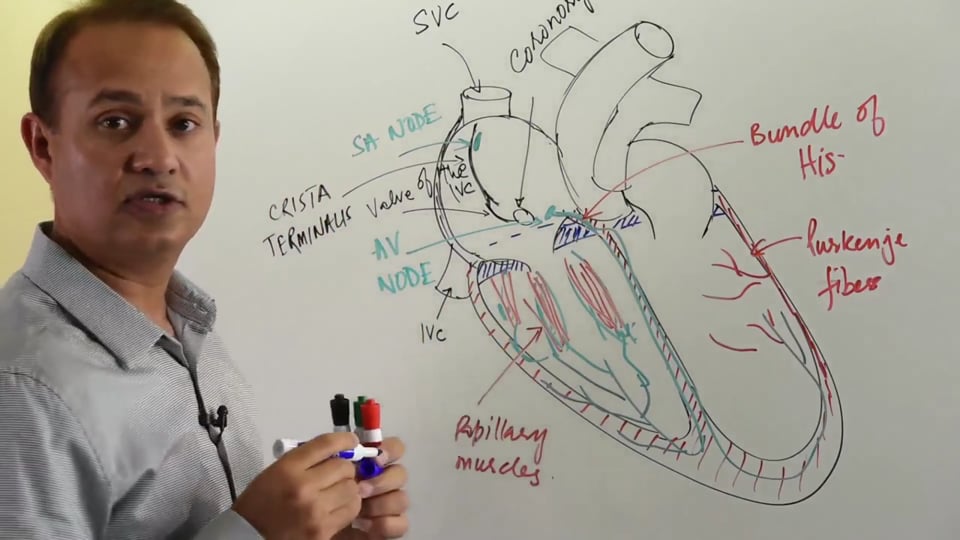
On the left side the remaining degenerating pieces of the sinus venosus become the coronary sinus. Right vitelline vein in future becomes the inferior vena cava. The common cardinal vein becomes the future superior vena cava. All these changes contribute to an increase in the size of right atrium since sinus venosus has also shifted there as part of its development. Anterior view of the right atrium shows that it's divided by the crista terminalis into a smooth and rough or trabeculated part. The trabeculated parts of right atrium and the right auricle are derived from the primitive atria. The smooth parts are derived from the primitive inflow tract which was sinus venosus. Crista terminalis is the landmark where parts of sinus venosus were absorbed into right atrium as parts of right atrial development. The lower part of the sinus venosus marks the valve of the inferior vena cava. Also there is an opening of coronary sinus which actually is the degenerated left sinus venosus draining into the right atrium.
DEVELOPMENT OF THE LEFT ATRIUM: Left atrial development is relatively not as complicated. Trabeculated part and the left auricle form a very small component of left atrium and they're derived from the primitive atrium. Majority of the left atrium is its smooth part which is derived from the primordial pulmonary trunk which gets absorbed as part of left atrial development. Primordial pulmonary trunk is actually a budding off of the left atrium. The primordial pulmonary turn initially grows and forms four branches. However, so much of the primordial pulmonary trunk is absorbed into the making of left atrium that its four branches end up opening directly into the left atrium.
In this video we will learn about :
1. Interatrial septum development.
2. Right atrium and sinus venosus.
3. Right atrium and pulmonary veins
4. Development of left atrium.
5. Smooth vs pectinate part of atrium.











Write A New Comment
0 Comments